Introduction
SBB technique: Satisfactory bone volume is an essential requirement for placing dental implants and achieving good aesthetic results.
In everyday practice, it is common to treat insufficient alveolar crests that may require surgical augmentation to position the implants correctly. SBB technique.
In cases where there are defects or significant bone atrophy, it is advised to use a bone augmentation restoration technique simultaneously or before placing implants. For this there are various techniques such as block grafts, guided bone regeneration or the Split Bone Block (SBB) SBB technique described by Dr. Khoury.
This technique consists of obtaining a bone block from the mandibular symphysis or branch, which is generally divided into two fine slices, ideally less than 0.5 mm thick, and stabilised with microscrews in the recipient bed, filling the gap created with autogenous bone particles. The literature has demonstrated that the SBB technique is a straightforward method with reliable clinical results for the horizontal bone augmentation of both maxillae1-3.
Case presentation
A case is presented below of a 55-year-old patient, with no medical
history of relevance, who came to the clinic for the permanent restoration of
the left superior maxilla.
After the pertinent examination, it was observed that the patient presented a fine narrow crest with some small bone defects,
and he was offered treatment to restore the alveolar crest, using autologous
bone, with the simultaneous placement of three implants that would later hold a
partial metal-ceramic restoration.
Surgical phase
The patient was given local anaesthesia with Articaine and a full-thickness flap was created to expose the superior maxilla.
Intraoperative calculations were made for the block length needed using a millimetre probe, measuring the maximum distance between the implants. The block was cut with a microsaw, and removed with the help of a chisel. Particulate bone was obtained with a bone scraper separately from the laminated block, directly from the mandibular branch. This was mixed with a minimal portion of xenograft to finish filling the gaps between the native bone and the laminate block. It was closed with two planes of sutures with single and horizontal mattress stitches.
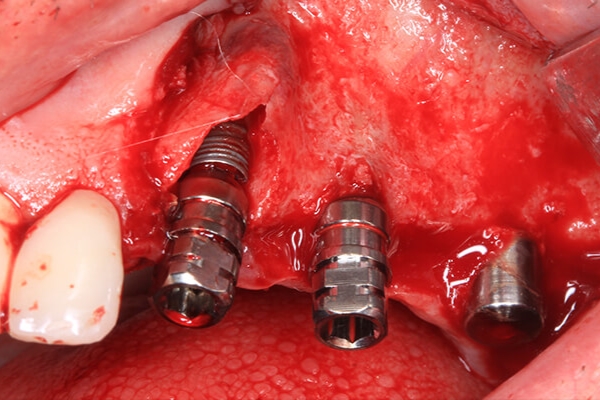
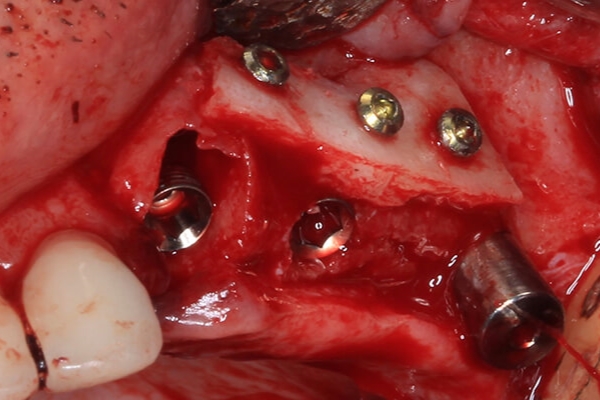
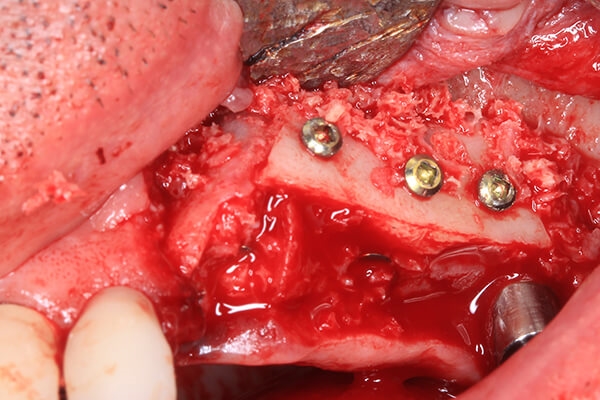
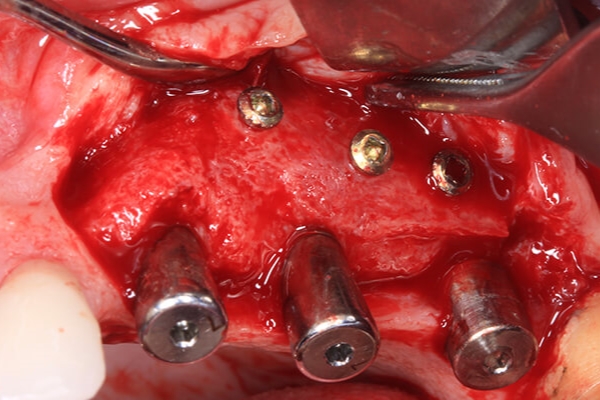
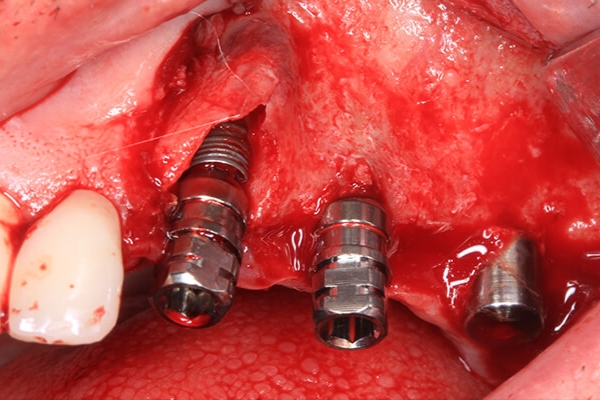
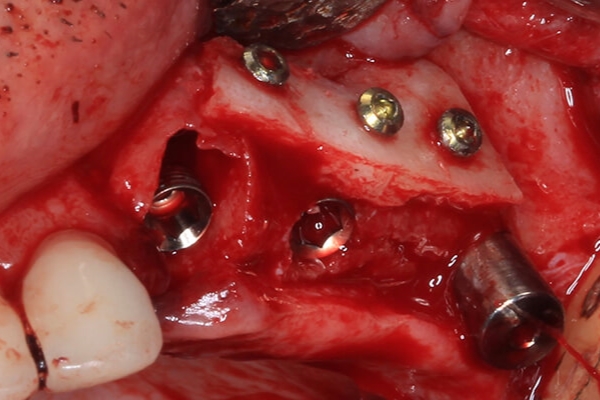
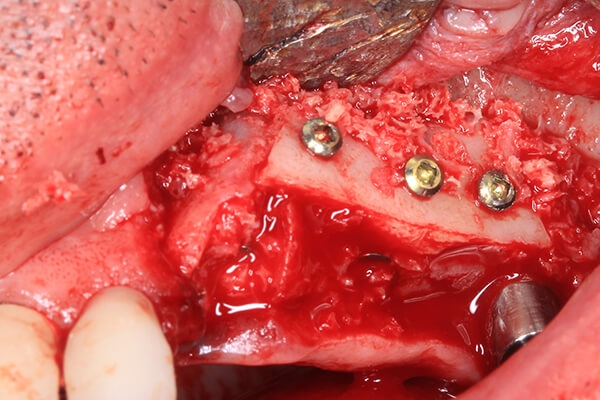
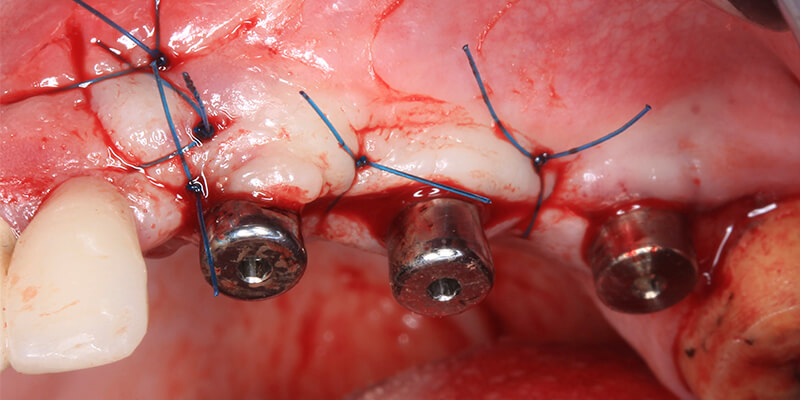
Three Biomimetic Ocean IC implants by Avinent were placed in accordance with the drilling procedure indicated. In the same surgery the maxilla was restored with autologous bone from the mandibular branch with a block. In this case we did not split the block of cortical bone from the mandibular branch. We slimmed it directly with a bone scraper and secured it to the native bone with osteosynthesis microscrews with a diameter of 1.2 mm to the wall of the alveolar crest, immobilising the graft. The remaining space was filled with blood and bone particulate from the patient, aiding quick revascularisation and regeneration of the bone as the graft was in direct contact with recipient bed.

Placement of the Biomimetic Ocean IC implants and details of the bone defect.Implants without transporter and details of the bone plate secured with osteosynthesis screws. Implantes sin transportador y detalle de la placa ósea fijada con tornillos de osteosíntesis. Autologous material recovered. Bone regeneration to fill gaps.

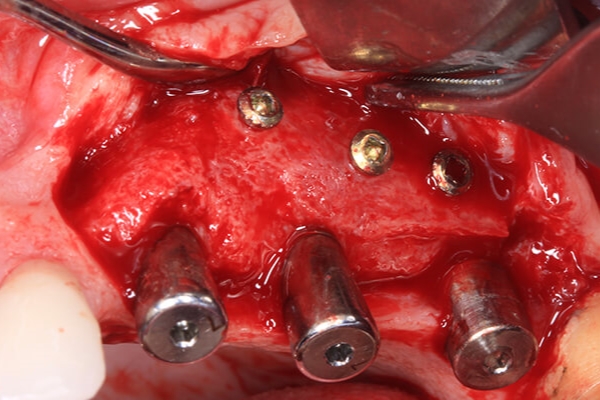
As good primary stability was achieved in the most distal implant, it was decided to place healing abutments with a height of 6 mm and to begin to shape the soft tissues.

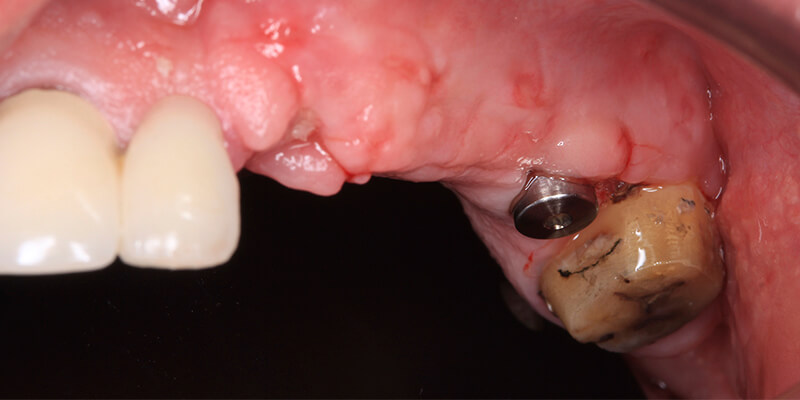
After 4 months, the area was reopened with a displaced flap of keratinised tissue from palatal to vestibular. Sufficient volume and quality of neoformed tissue was observed, as was the correct position of the implants that would facilitate the placement of the prosthetic restoration. We also removed the screws that attached the graft.
Details of regenerated bone volume. 
Closing suture.
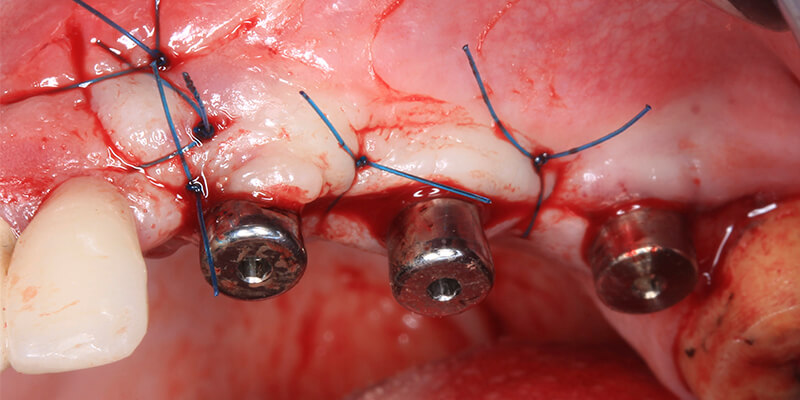
Two weeks after the second intervention, three straight transepithelial abutments by Avinent were placed to permit better insertion of the multiple restoration, facilitating passivity and distancing the connection of the implants for better biological seal and reduced invasion of the soft tissues.

Prosthetic phase
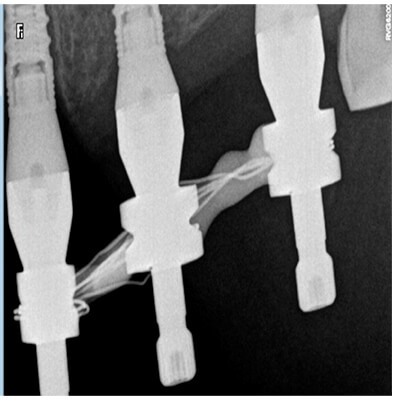
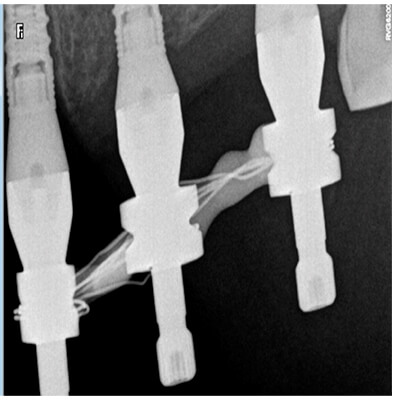
Impressions were taken with conventional open tray techniques splinting the impression transfers.
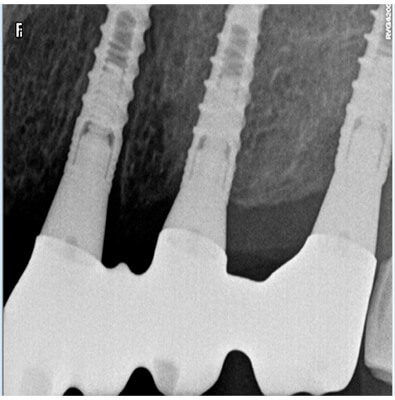
Once the definitive metal-ceramic prosthesis had been designed and manufactured, the functional loading of the implants was carried out.
The restoration was connected to the transepithelial abutments with a torque of 15 Ncm and the patient’s occlusion was adjusted.

Details of the impression transfers on splinted transepithelial abutments.
Details of the adjustment of the partial prosthesis on the transepithelial abutments.
At first it was planned to replace the patient’s previous prosthesis along with the implant-mounted partial prosthesis to improve the final aesthetics of the anterior sector. However, once the posterior defect had been corrected, the patient did not wish to continue with the aesthetic treatment.

Conclusion
Thanks to bone regeneration techniques such as the Split Bone Block or SBB described by Dr. Khoury, a horizontal augmentation of the alveolar crest can be achieved with sufficient volume to place implants in an atrophic maxilla with a good long-term result.
Thanks to Ana Fernandez of the Oporto Dental clinic for her collaboration in the prosthetic restoration.
Dr. Constantino Colmenero

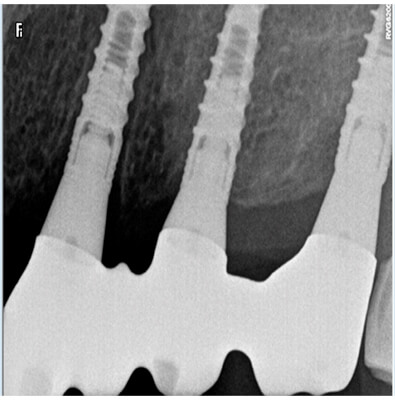
Placement of the Biomimetic Ocean IC implants and details of the bone defect. Implants without transporter and details of the bone plate secured with osteosynthesis screws. Autologous material recovered. Bone regeneration to fill gaps. X-ray control of the bone regeneration and the implants placed. Details of regenerated bone volume. Closing suture.
Closing suture.Healing of the soft tissue covering the Avinent uniblock transepithelial abutments.
Details of the impression transfers on splinted transepithelial abutments.Details of the adjustment of the partial prosthesis on the transepithelial abutments. Definitive partial prosthesis in the mouth.




Bibliografía
1 Khoury F, Doliveux R. The Bone Core Technique for the Augmentation of Limited Bony Defects: Five-Year Prospective Study with a New Minimally Invasive Technique. Int J Periodontics Restorative Dent. 2018 Mar/Apr;38(2):199-207
2 Khoury F, Hidajat H. Secure and effective stabilization of different sized autogenous bone grafts. European Journal of Oral Surgery. Vol. 2 n. 3 2011
3 Khoury F, Hanser T. Mandibular bone block harvesting from the retromolar region: a 10-year prospective clinical study. Int J Oral Maxillofac Implants. 2015 May-Jun;30(3):688-97