Introduction
After a tooth is lost, a number of dimensional changes will occur in the alveolar bone and, consequently, in the soft tissues, frequently causing defects in the alveolar ridge that can hinder or impede good implant positioning. It can also prevent us from achieving acceptable results from an aesthetic point of view, especially in the anterior sector. Socket preservation.
To prevent and treat these defects, there are different techniques that aim to preserve or increase the hard and/or soft tissues. Slight defects can generally be resolved by augmenting the soft tissues. Nevertheless, in cases with significant bone loss or where the treatment includes implant-supported prostheses, the combination of various techniques at different stages may be necessary. Socket preservation.
Case presentation
Male patient, 51 years of age, with no medical history of interest, consulted the clinic due to a work incident in which he received a strong blow to the upper incisors.
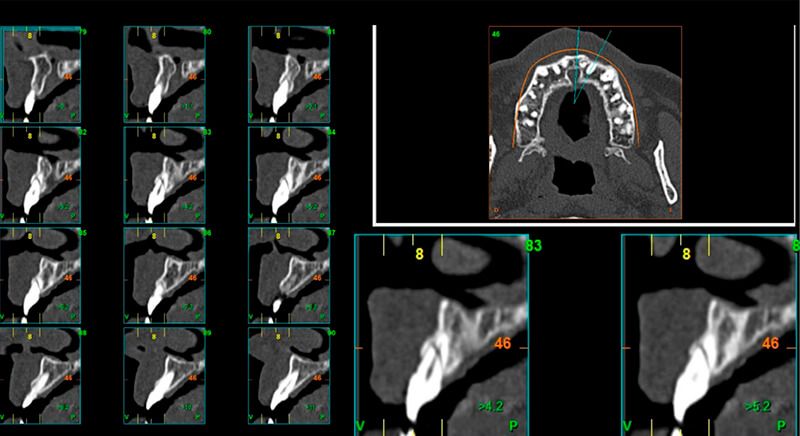
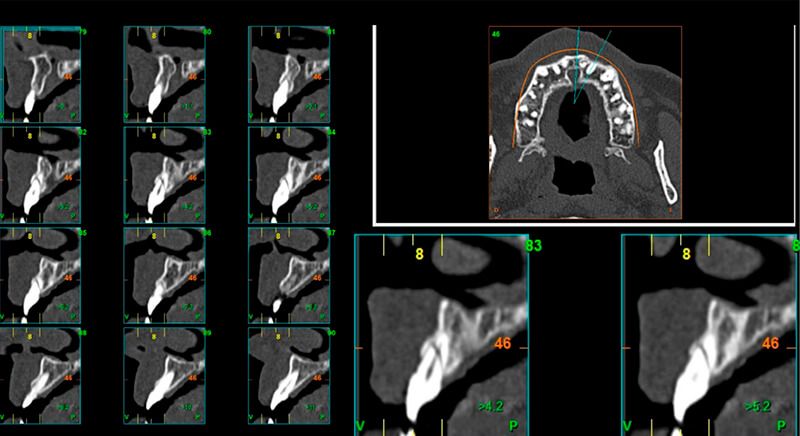
As result of an exhaustive examination a fracture of tooth 1.1 was detected, and although at first a fracture of 2.1 was not observed, it did present movement. Finally, the CT images revealed a radicular apical fracture of tooth 2.1 that meant the tooth could not be saved.


X-ray images of the initial status X-ray images of the initial status

Treatment plan
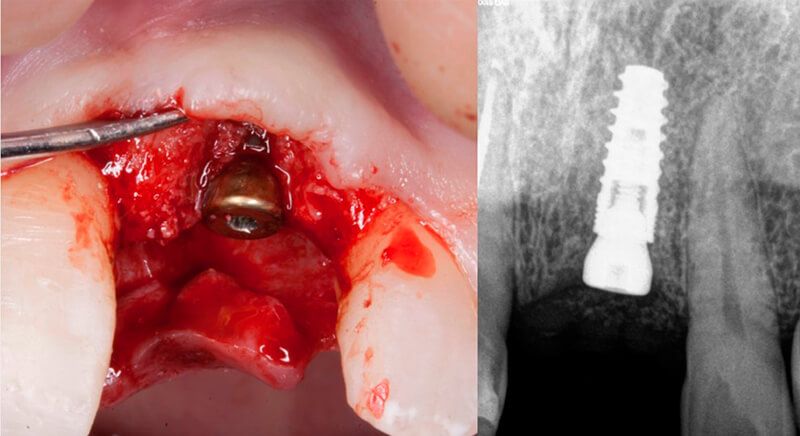
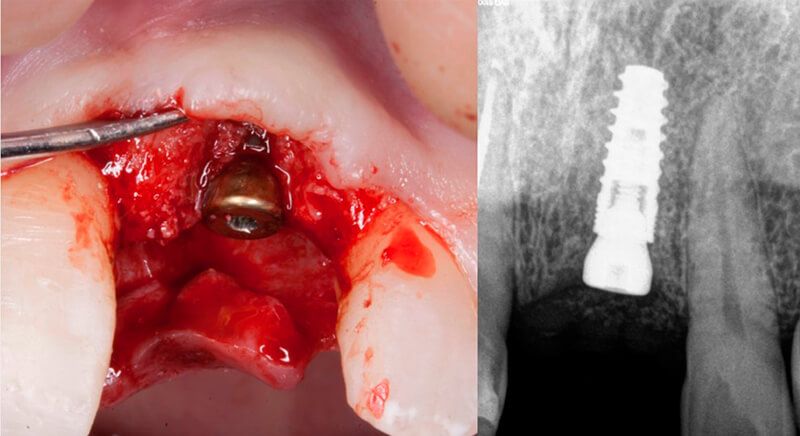
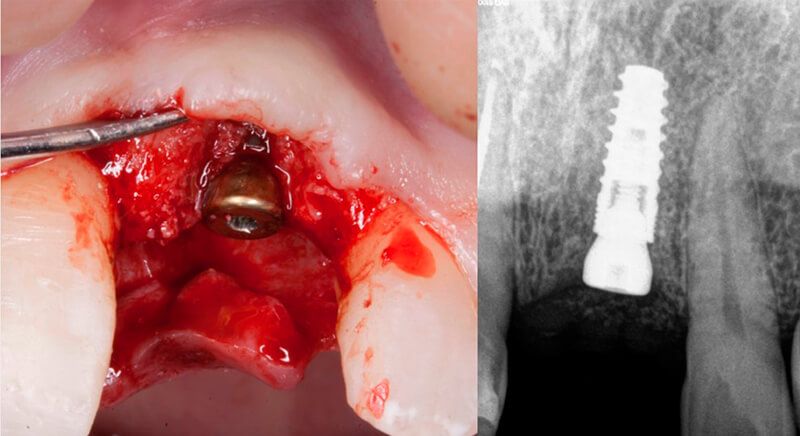
It was decided to reconstruct tooth 1.1 and perform endodontic work up to the fracture line of tooth 2.1 so it could be maintained provisionally, but the patient was very uncomfortable and unable to chew in this area so it was finally decided to extract both the coronal part and the fractured apex of tooth 2.1.
Details of the reconstructed tooth Details of the reconstructed tooth


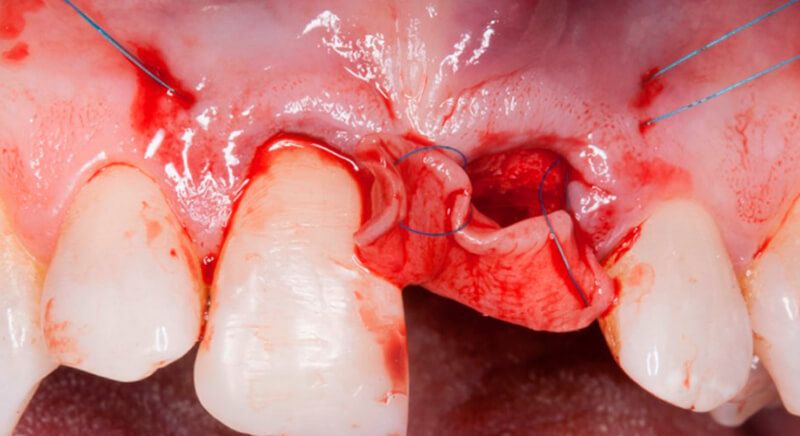
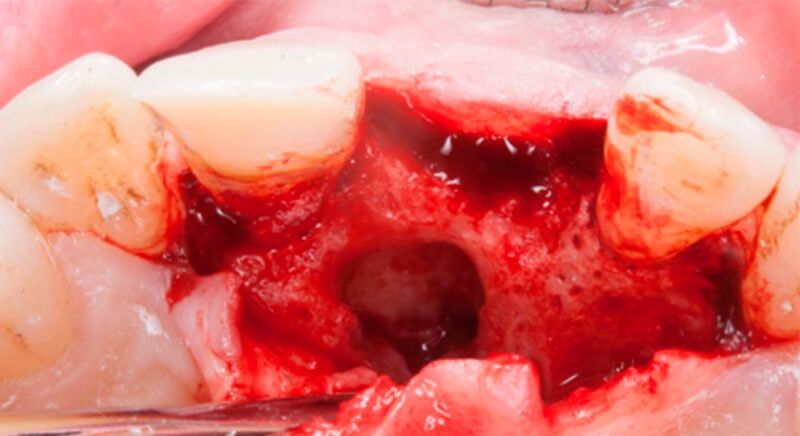
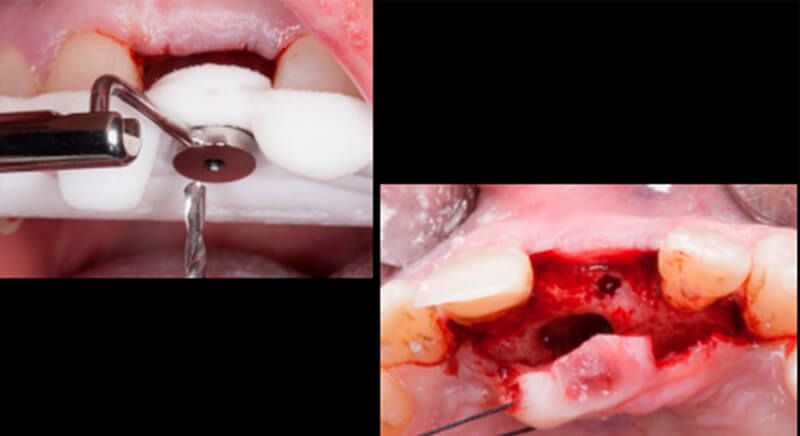
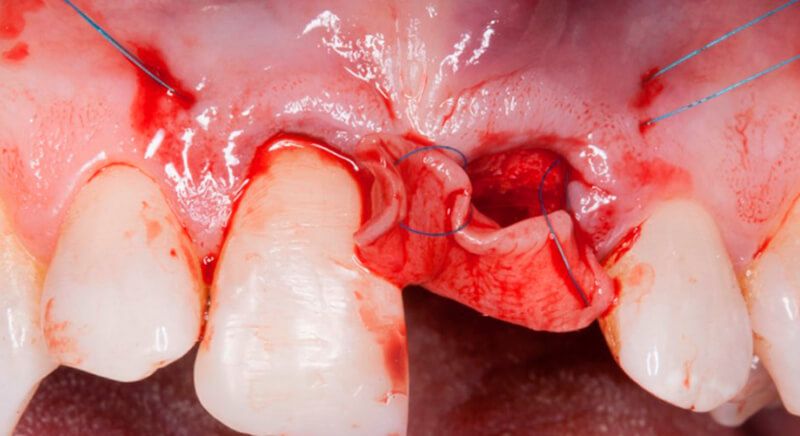
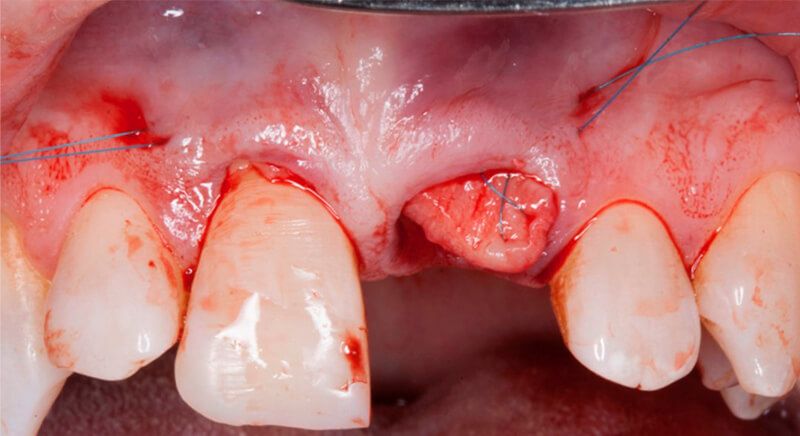
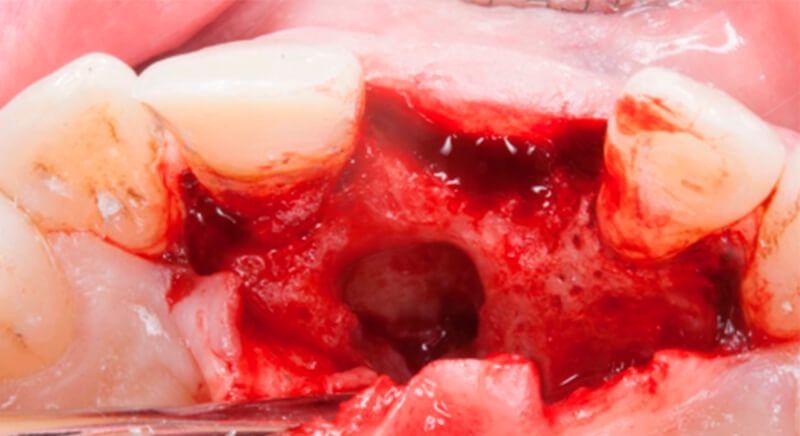
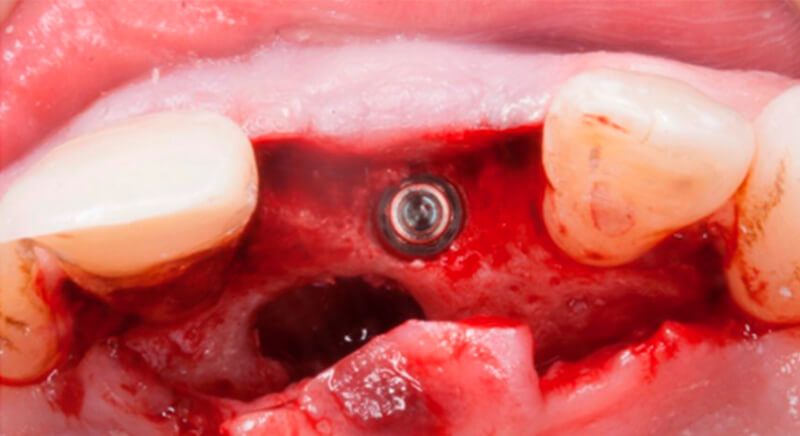
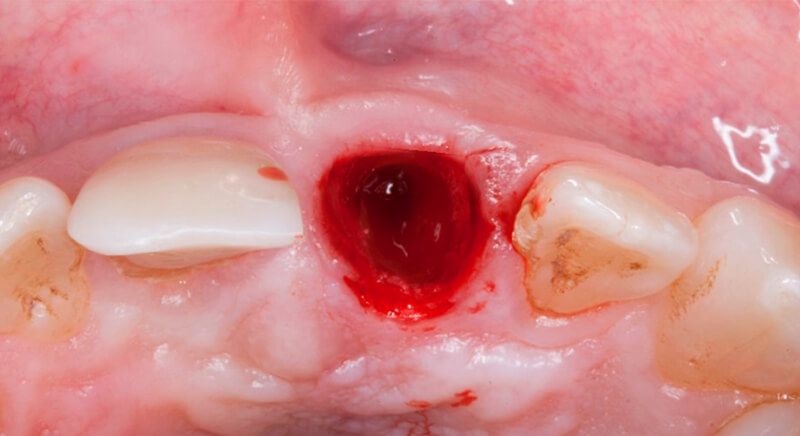
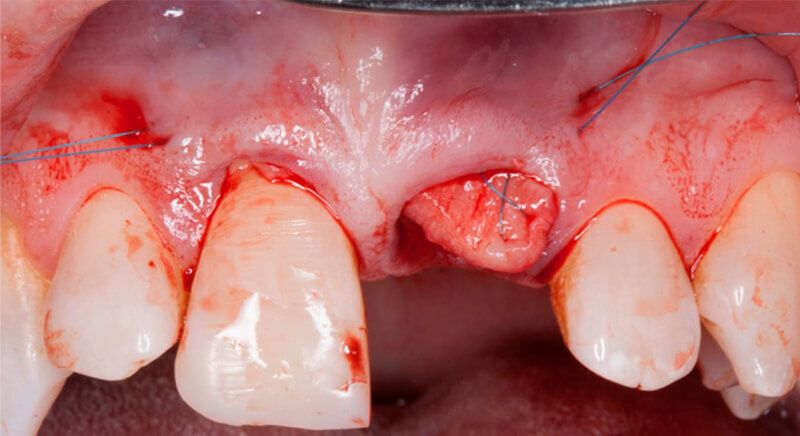
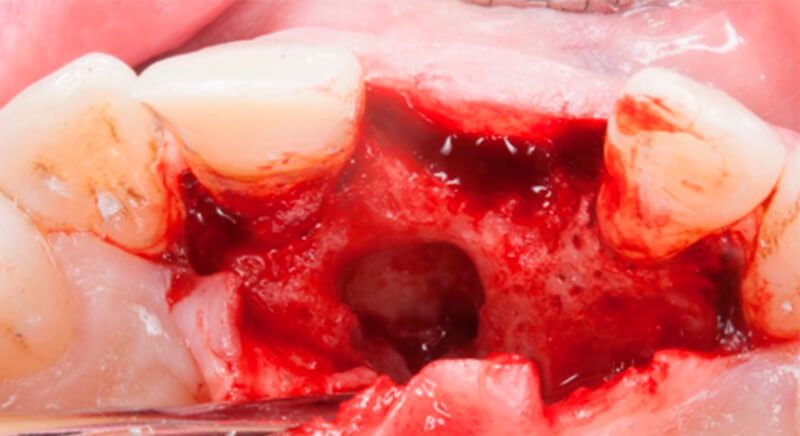
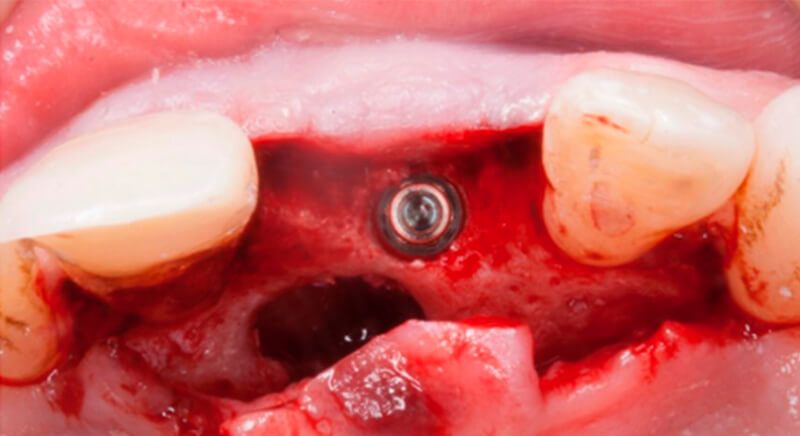
Sequence of images during the extraction of tooth 2.1. Sequence of images during the extraction of tooth 2.1. Sequence of images during the extraction of tooth 2.1. Sequence of images during the extraction of tooth 2.1.



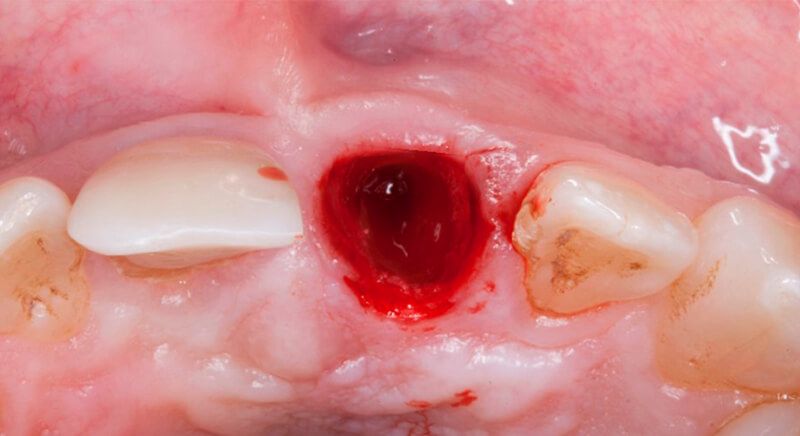
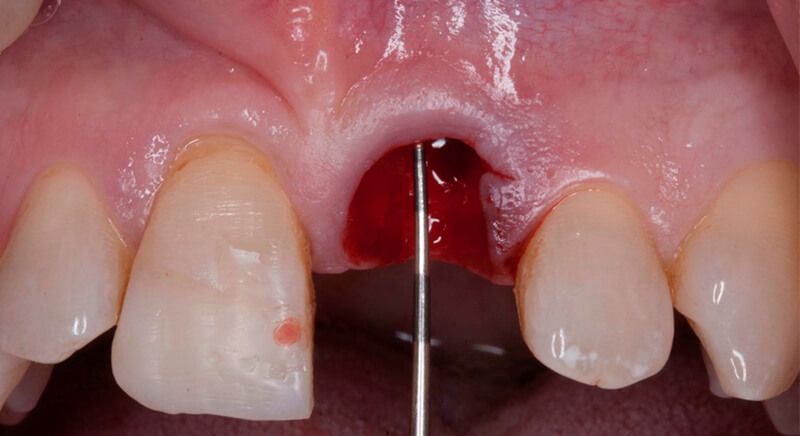
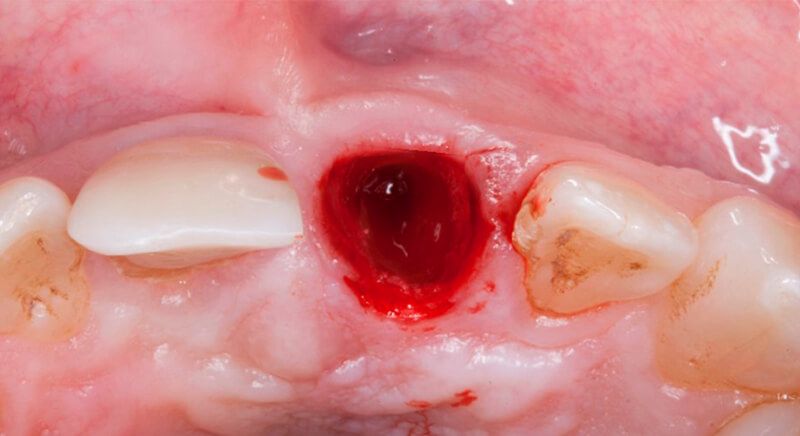
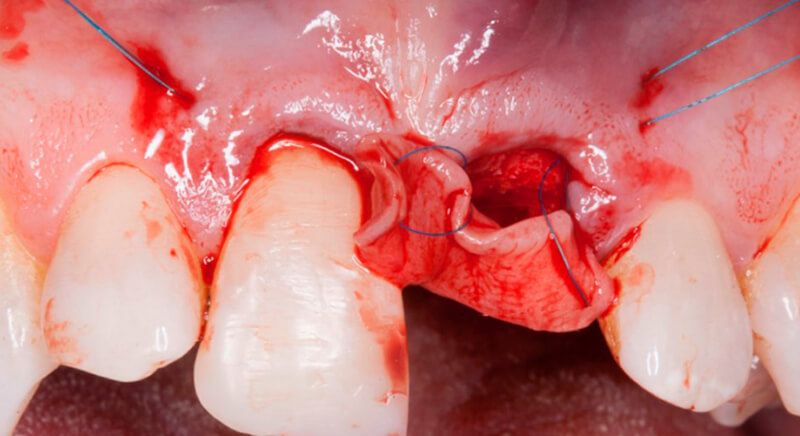
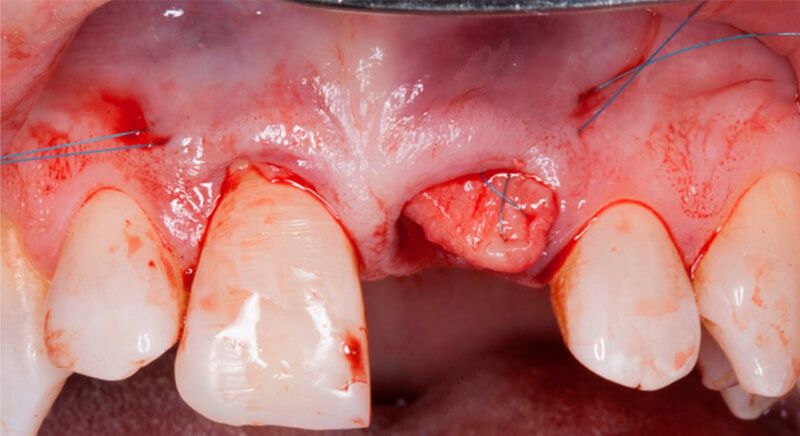
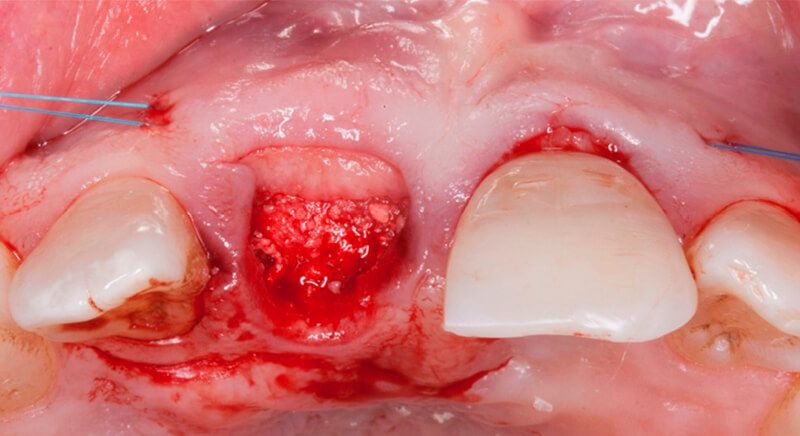
Once tooth 2.1 had been extracted, it was decided that it was not advisable to place an implant immediately as the bone conditions were not ideal and the gum did not have sufficient thickness. We opted for a treatment to preserve the socket and to delay implant insertion.
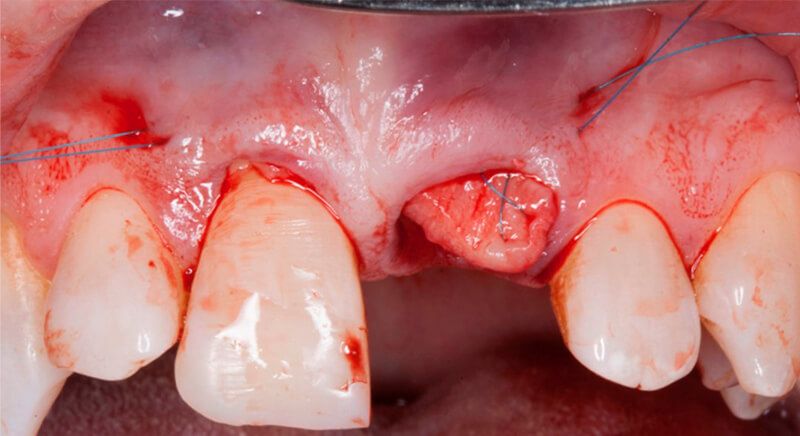
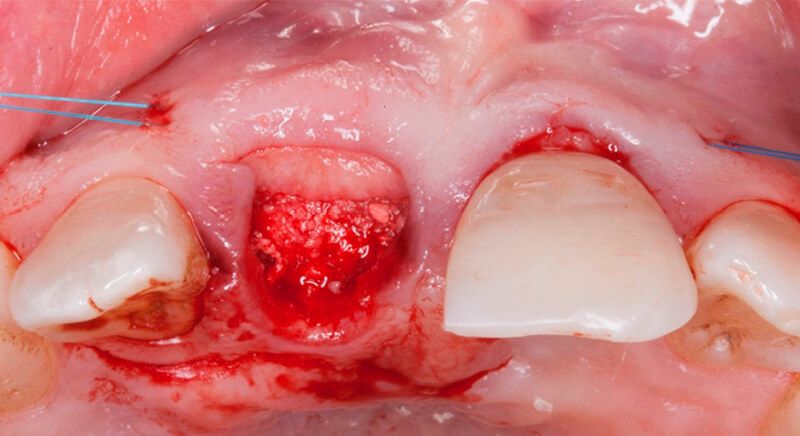
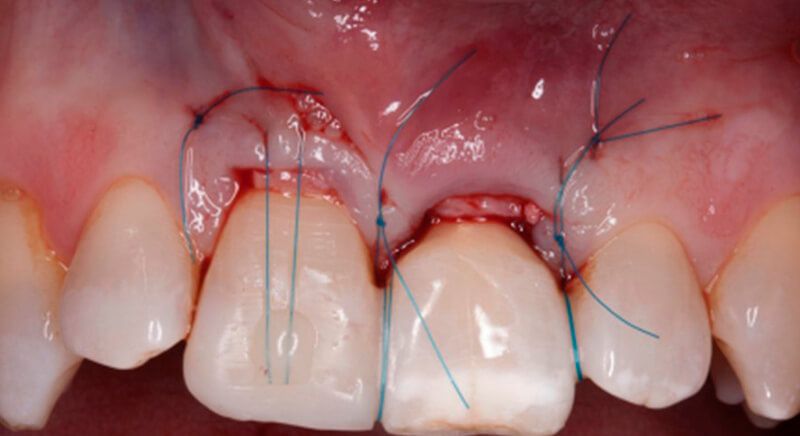
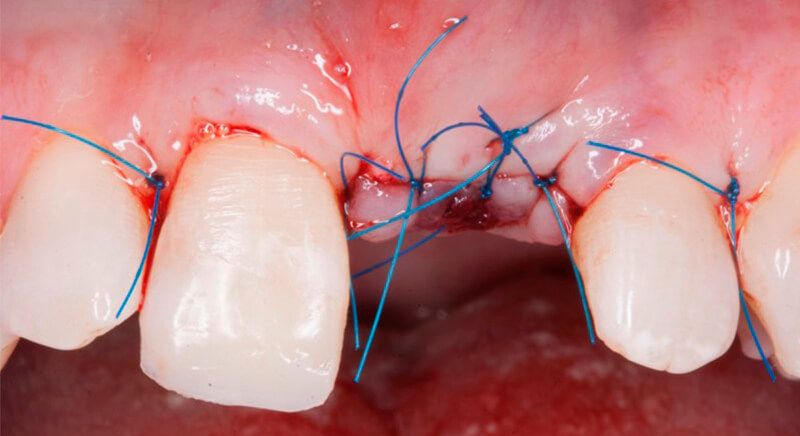
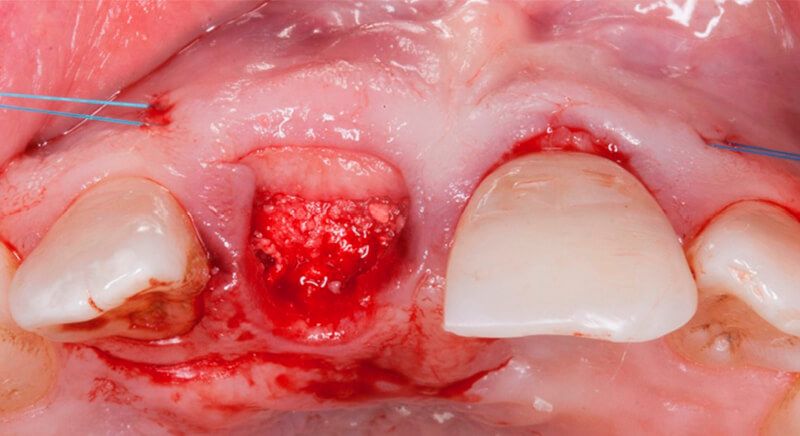
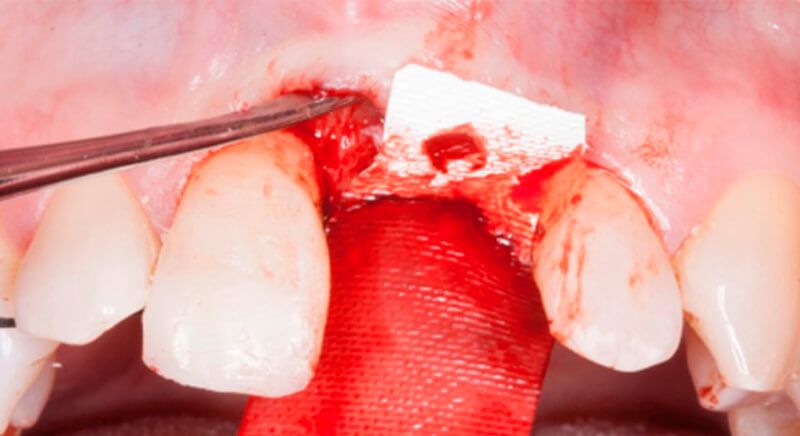
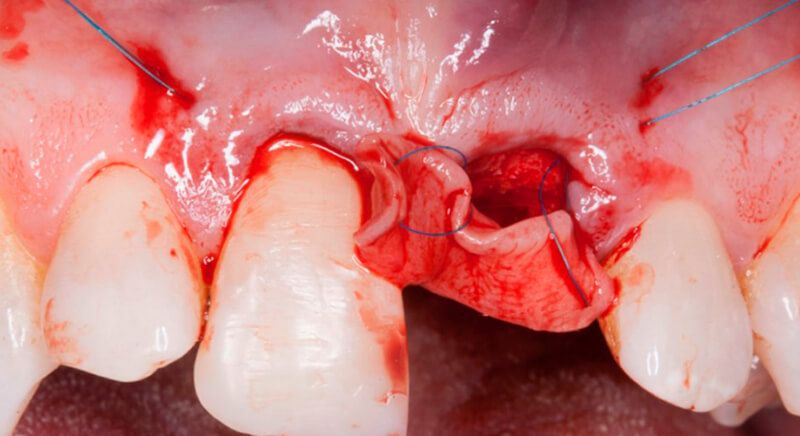
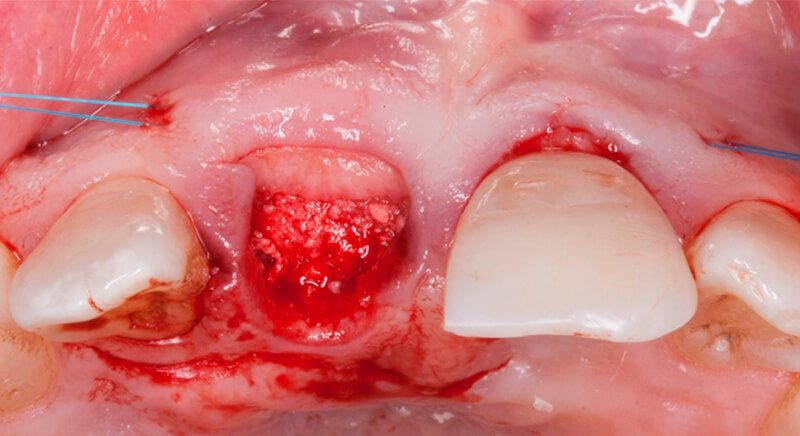
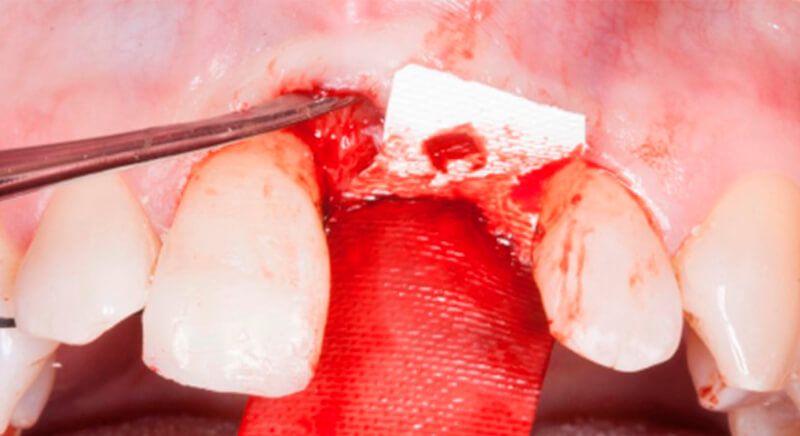
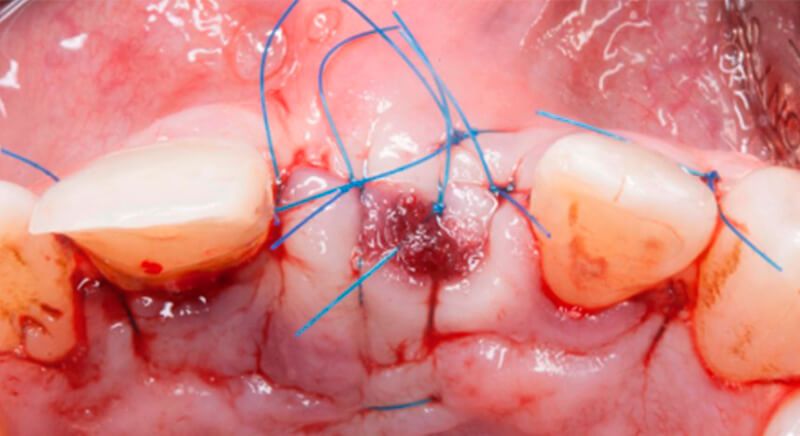
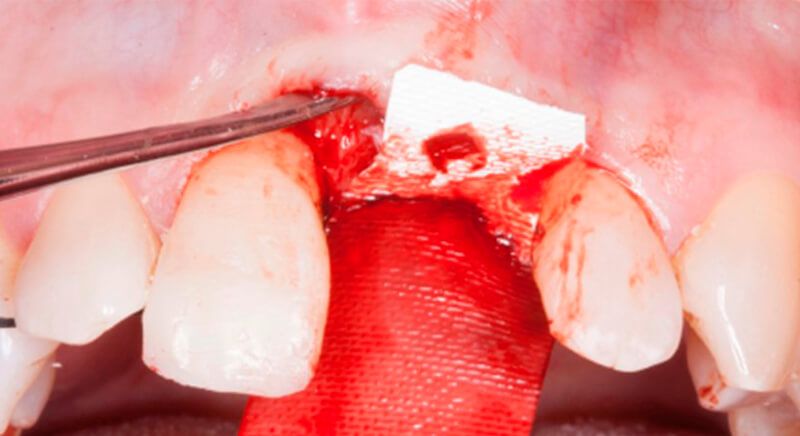
The socket was filled with a xenograft after the extraction and a graft of connective tissue was placed in the vestibular area of the two upper central incisors.
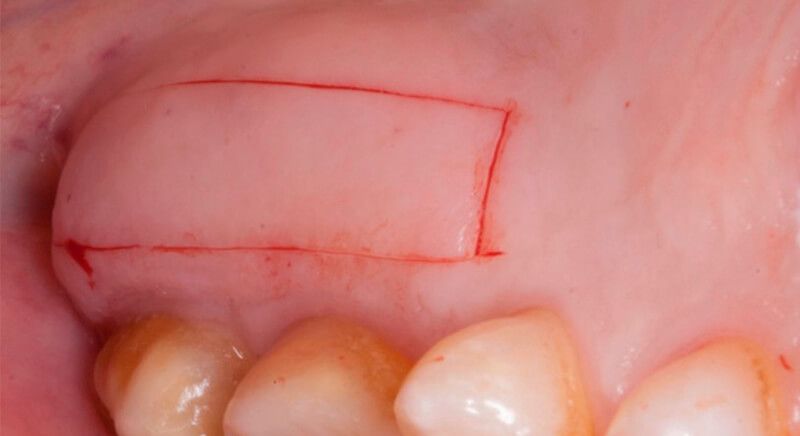
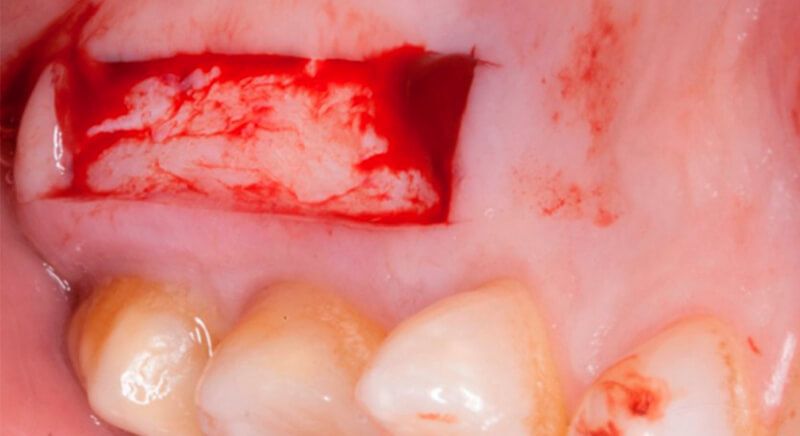
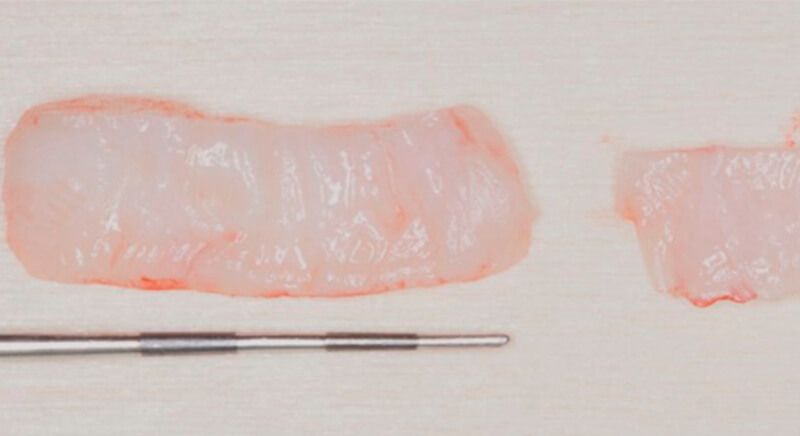
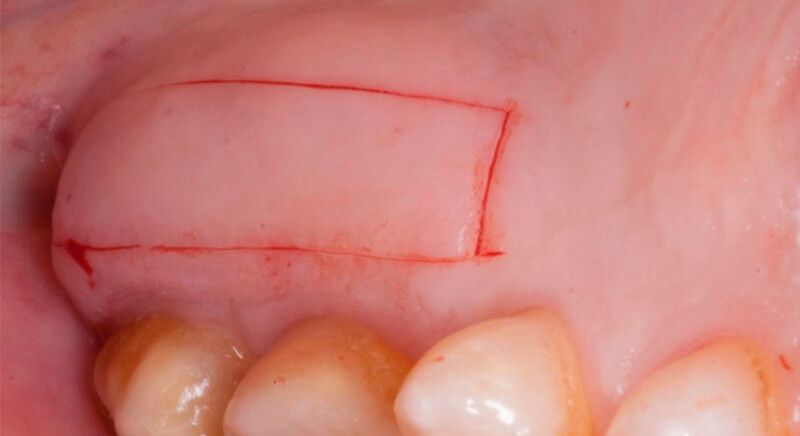
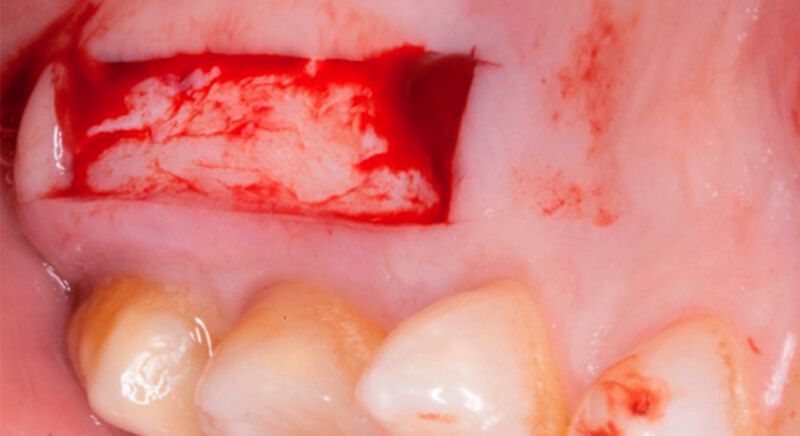
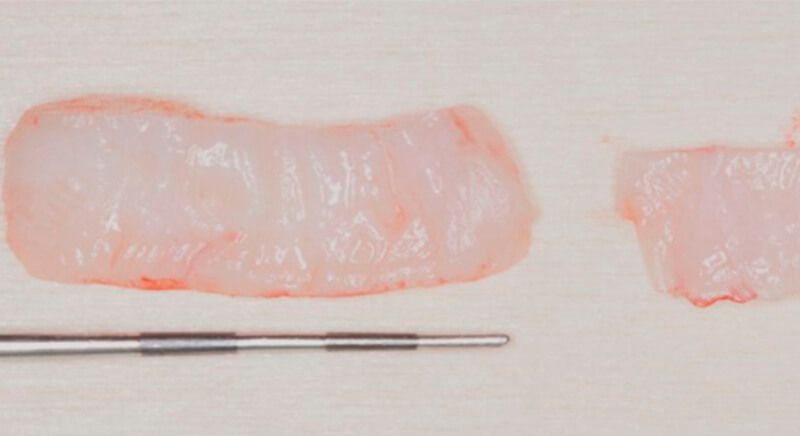
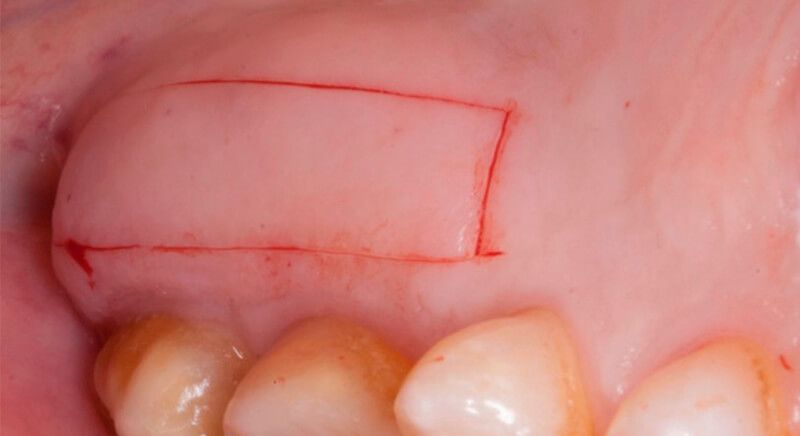
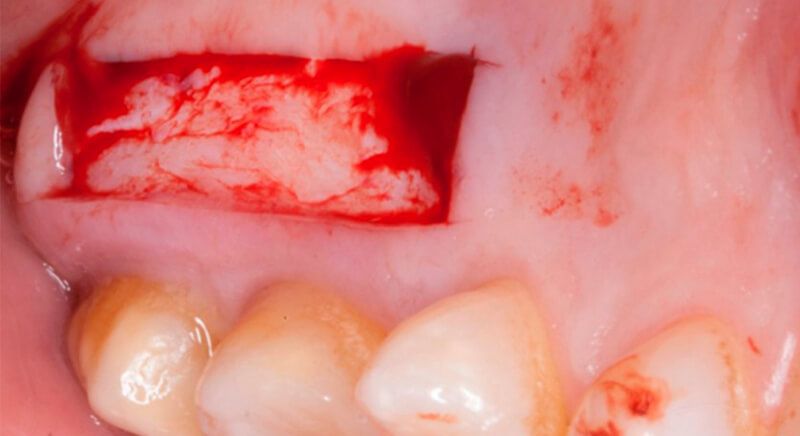
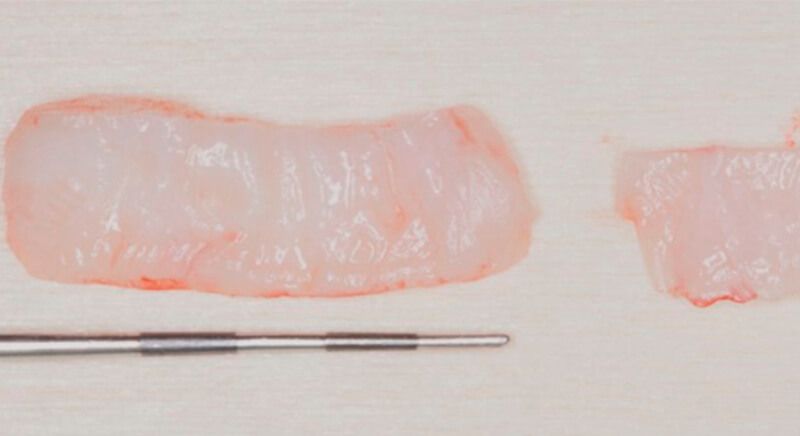
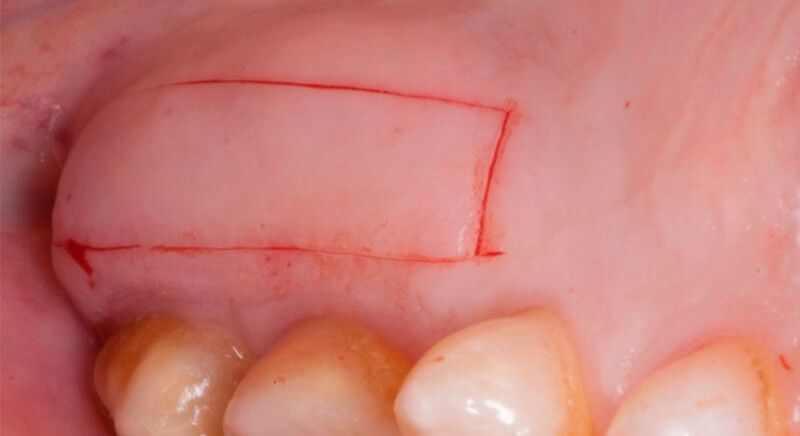
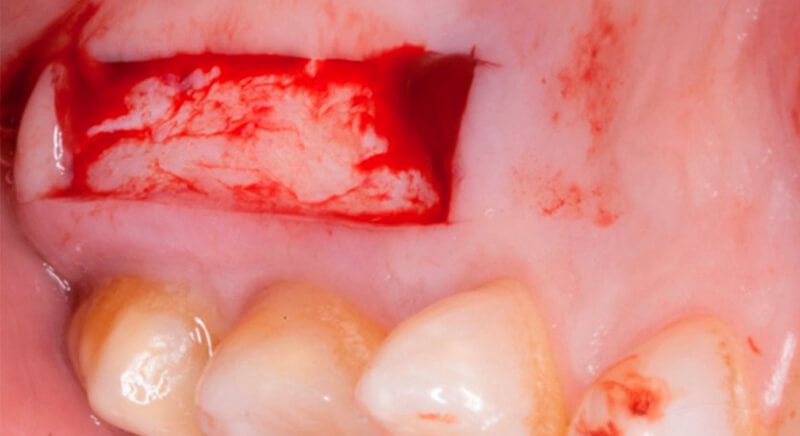
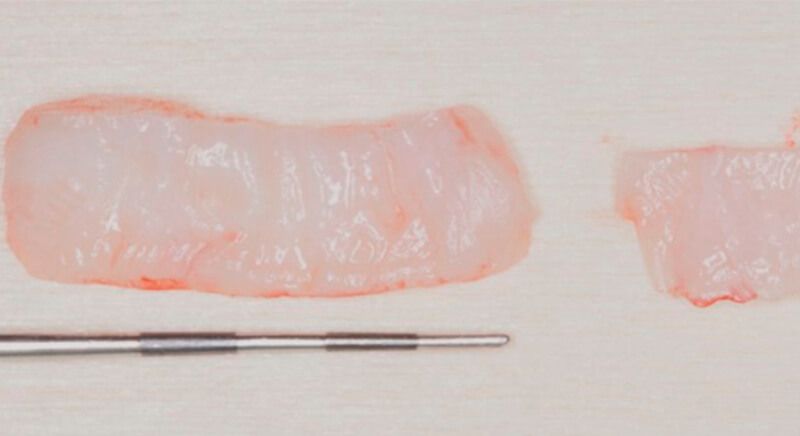
The tissue with epithelium was taken from the palate and de-epithelialized outside of the mouth. This obtains a lamina propria graft with better density and quality than if it were obtained with a single incision to the palate.
Placing the xenograft Incision in the donor area of the palate Incision in the donor area of the palate De-epithelialized lamina propria graft

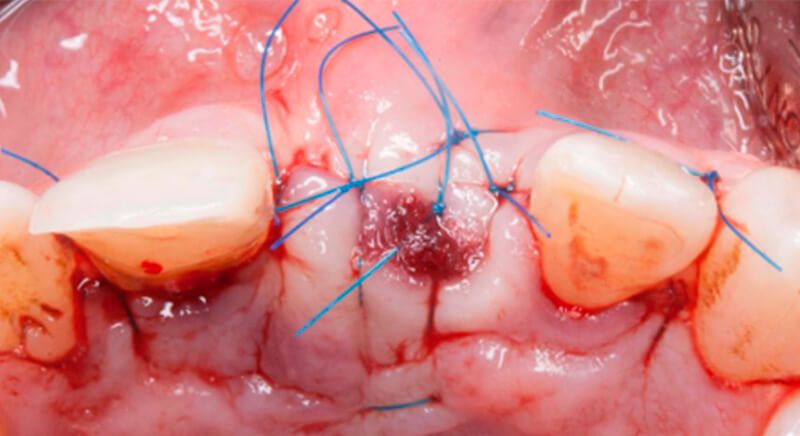
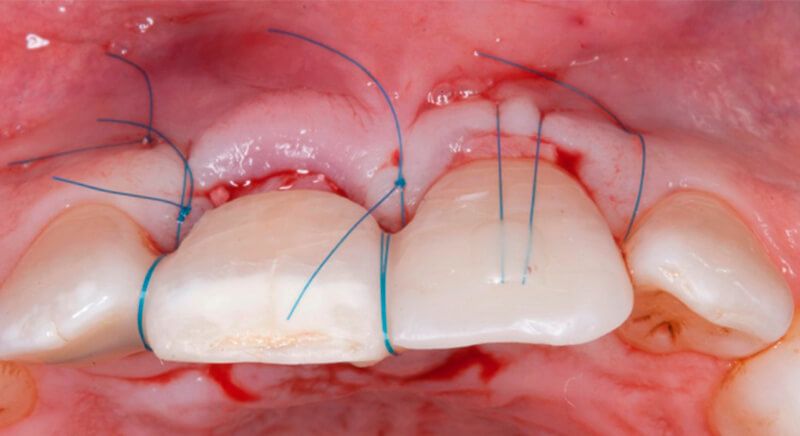
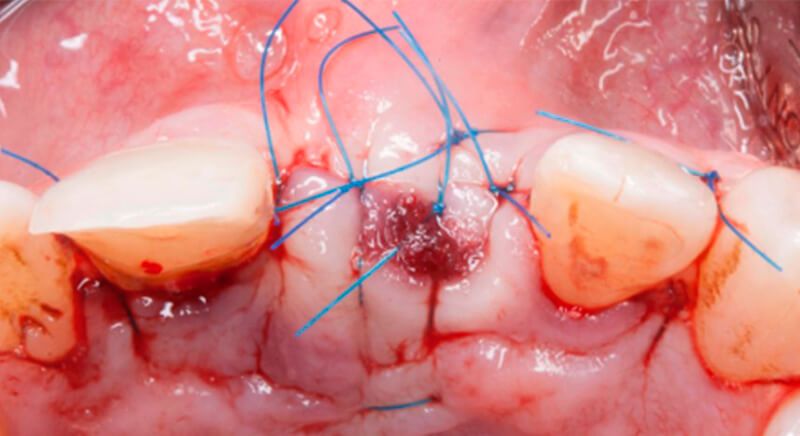
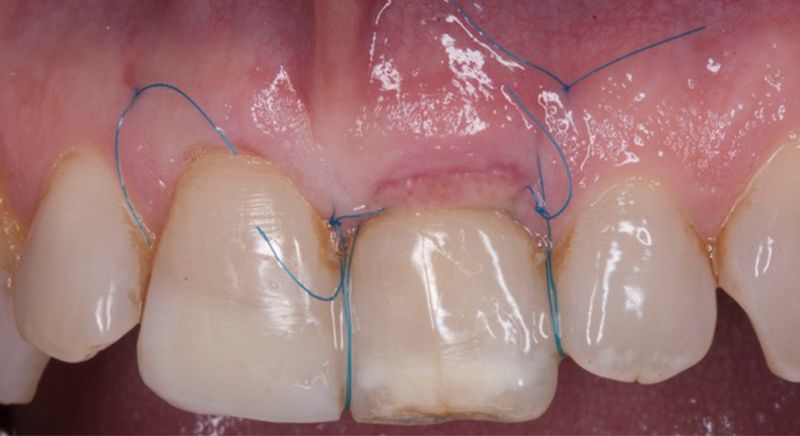
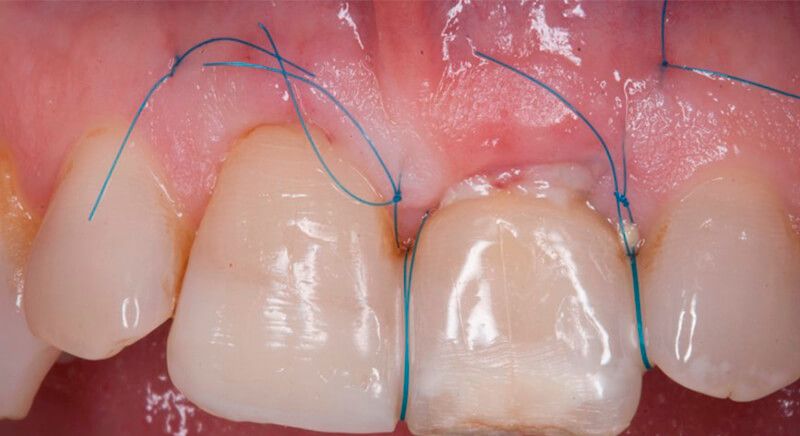
Sequence of the socket preservation technique and placement of the connective tissue graft
Sequence of the socket preservation technique and placement of the connective tissue graft
Sequence of the socket preservation technique and placement of the connective tissue graft
Sequence of the socket preservation technique and placement of the connective tissue graft
Sequence of the socket preservation technique and placement of the connective tissue graft


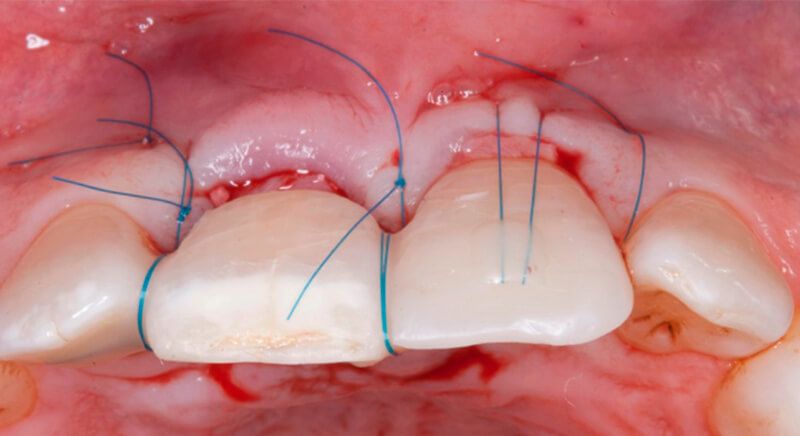
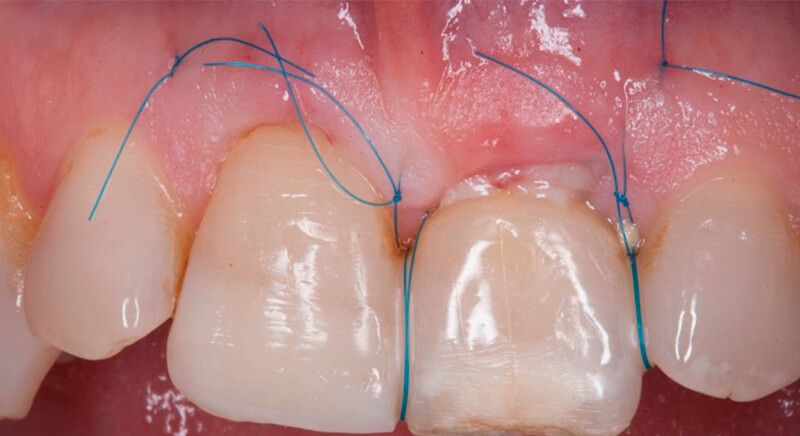
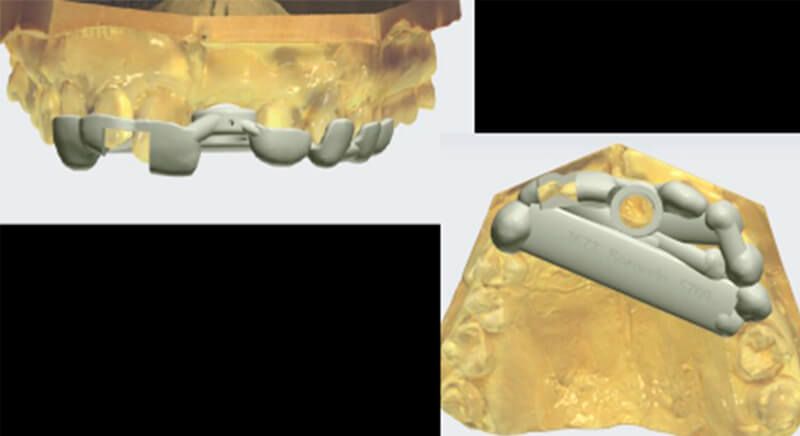
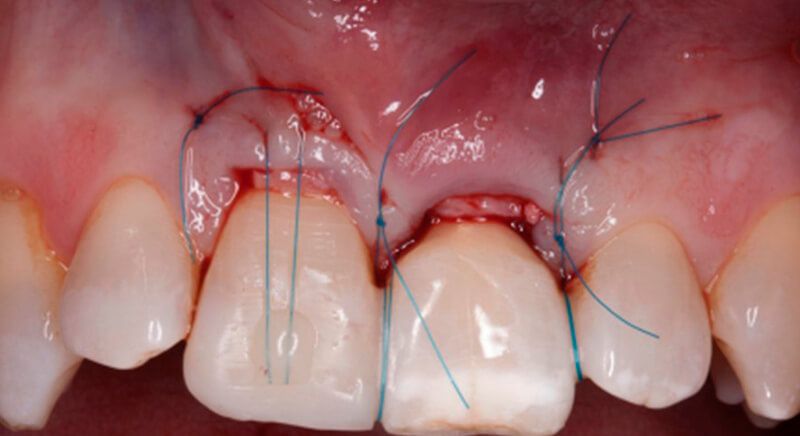
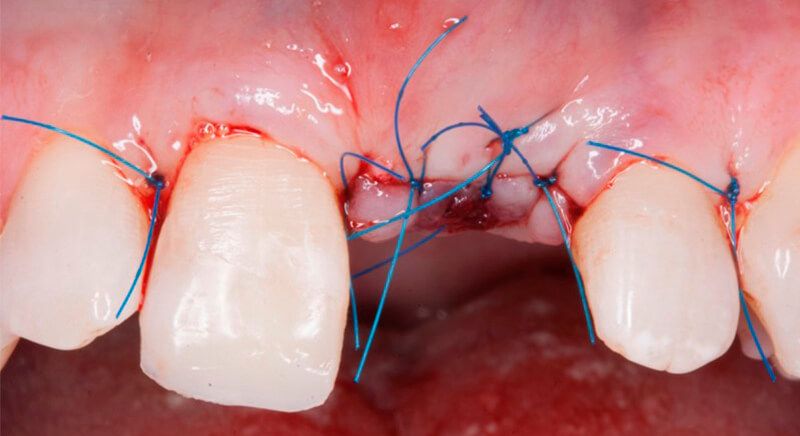
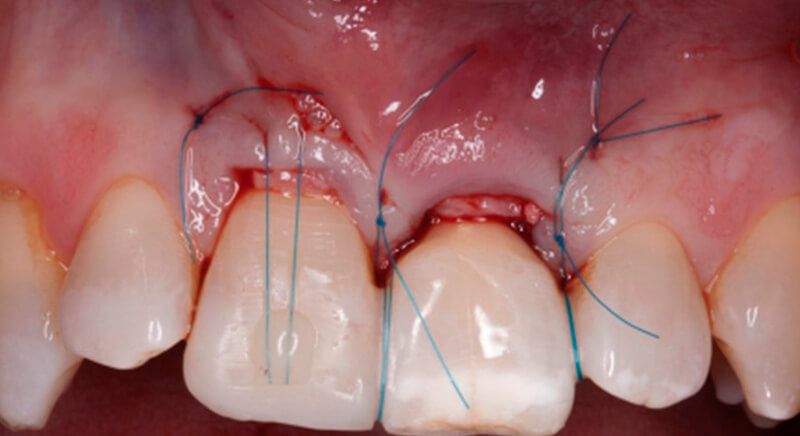
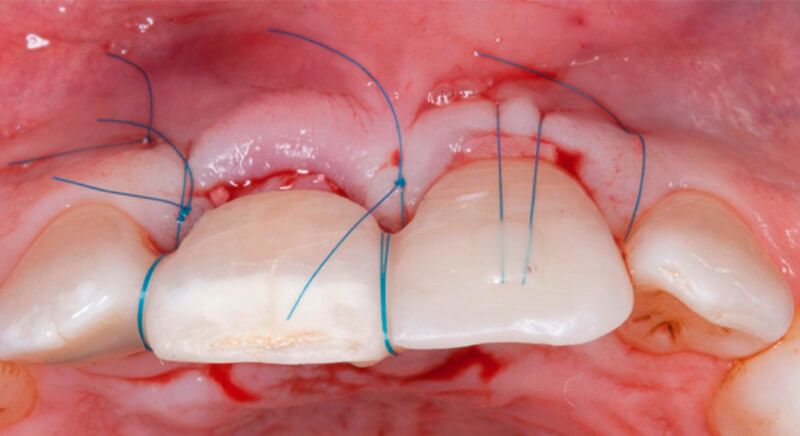
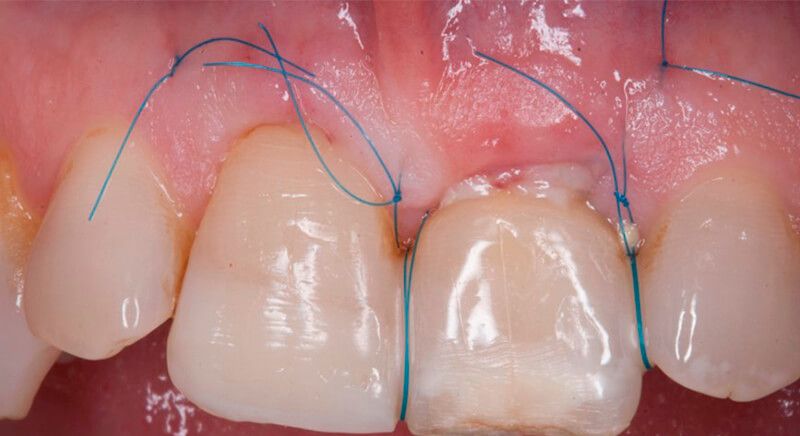
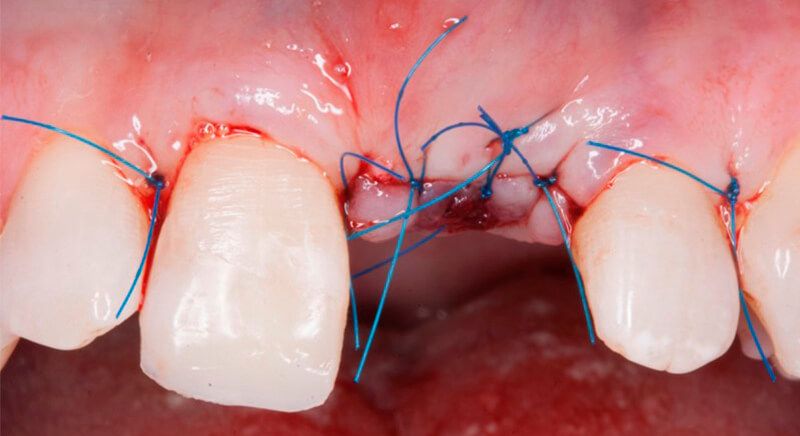
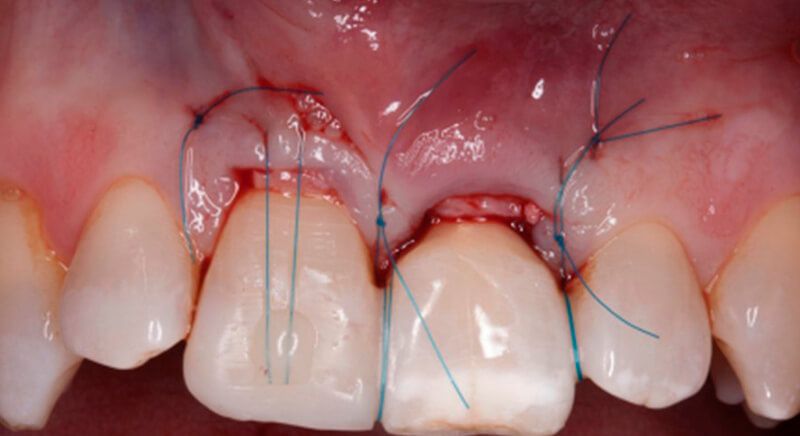
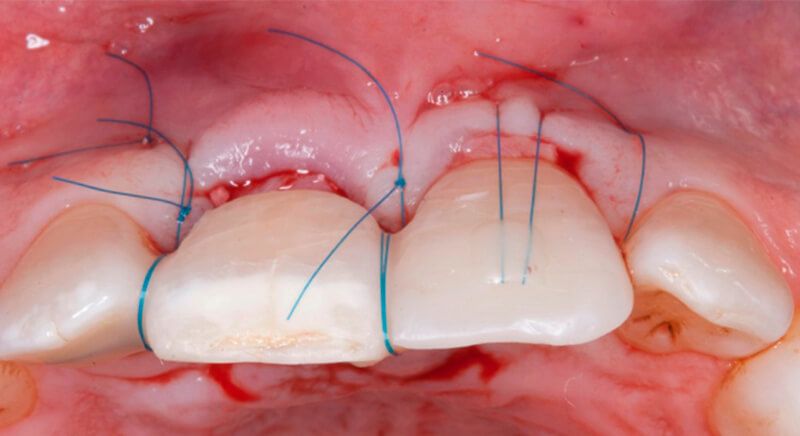
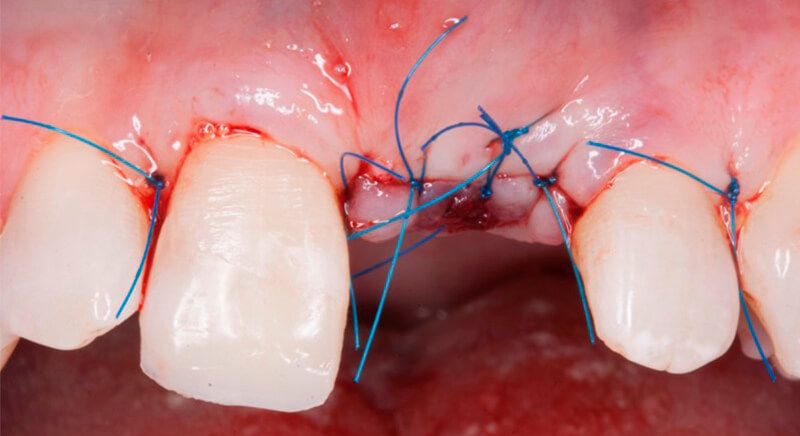
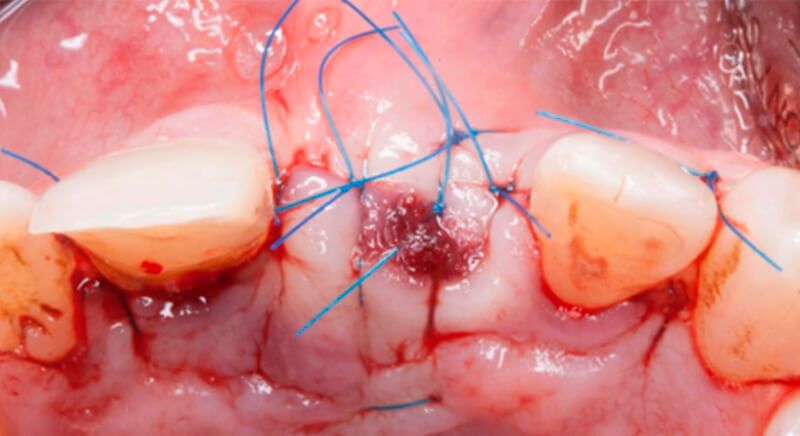
Placing the aesthetic Maryland-type immediate-load provisional and suturing the graft
Placing the aesthetic Maryland-type immediate-load provisional and suturing the graftX-ray of the regeneration and the provisional without load

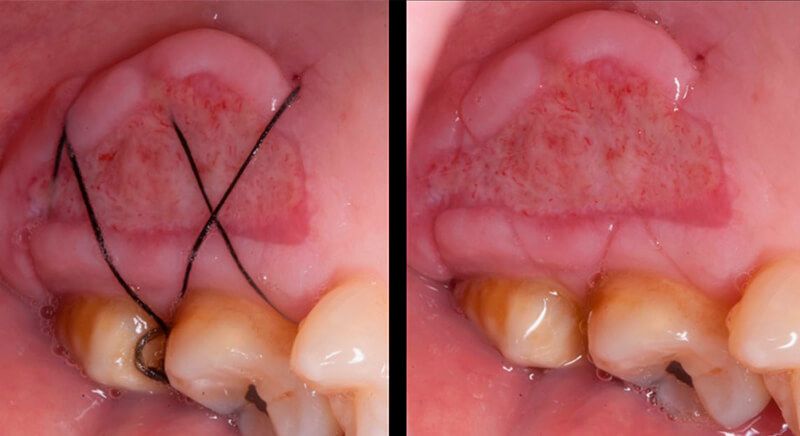
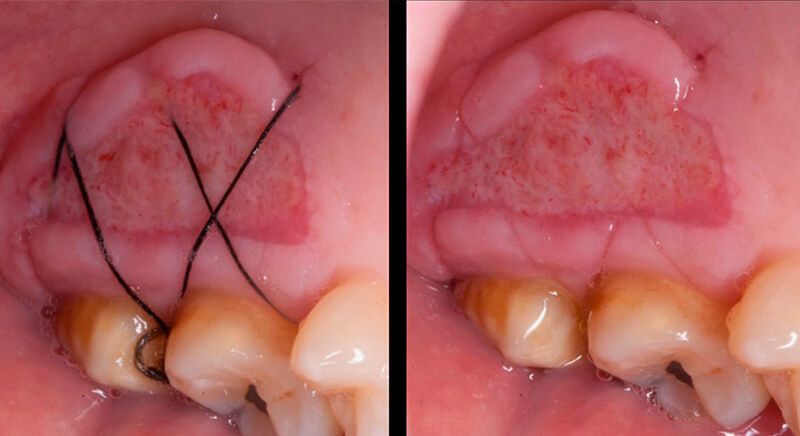
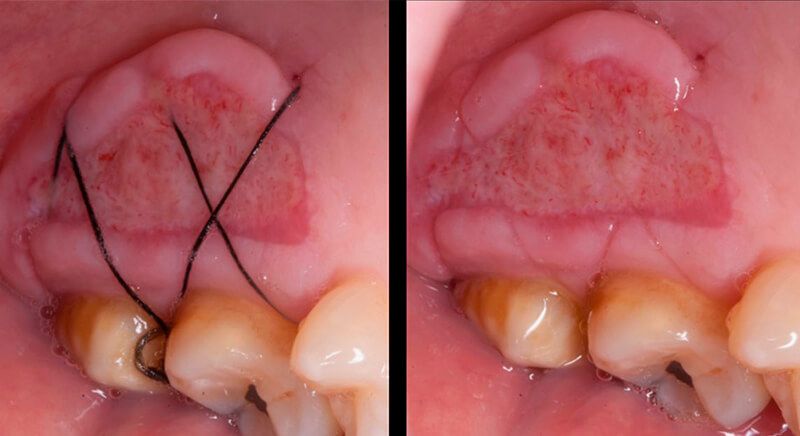
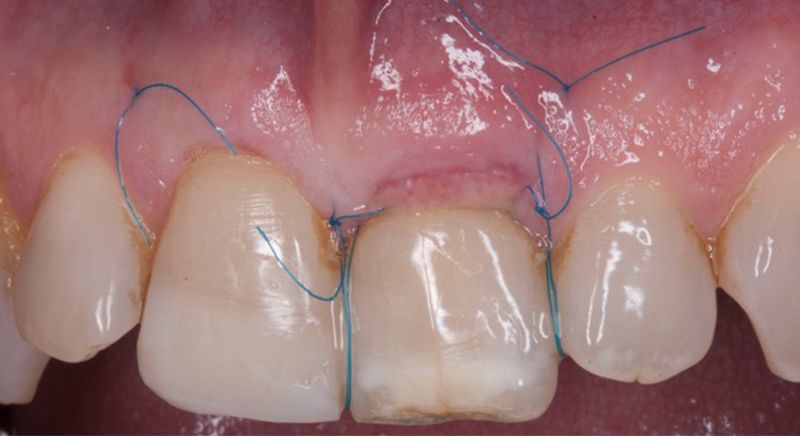
Healing of the donor and receiving areas 7 days after the mucogingival surgery
Healing of the donor and receiving areas 7 days after the mucogingival surgery
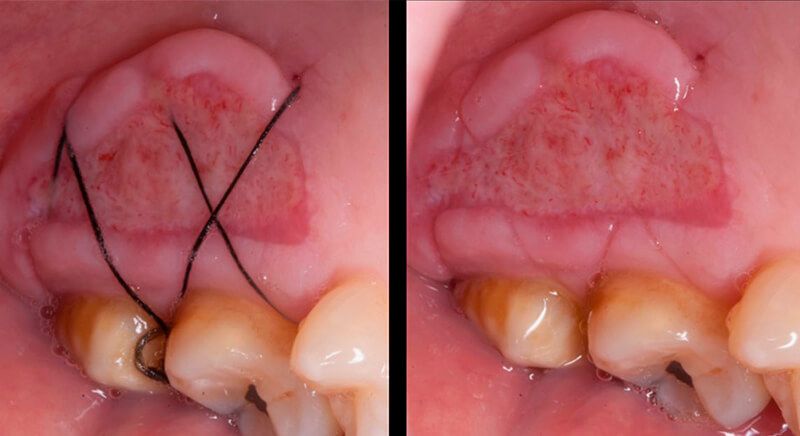
State of the tissues after 15 days Final removal of the sutures

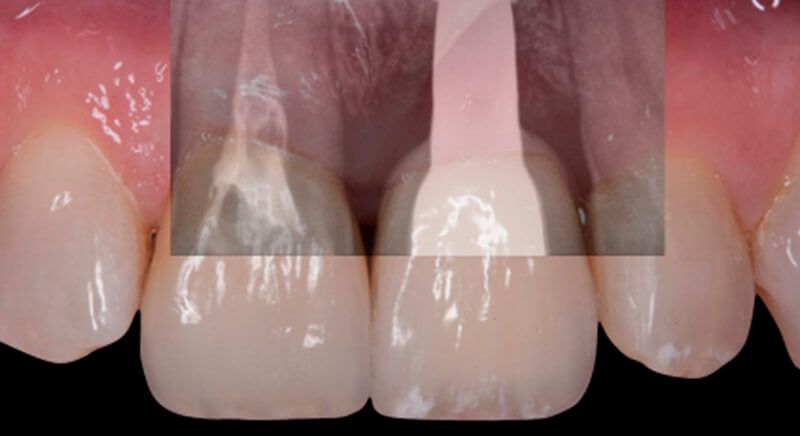
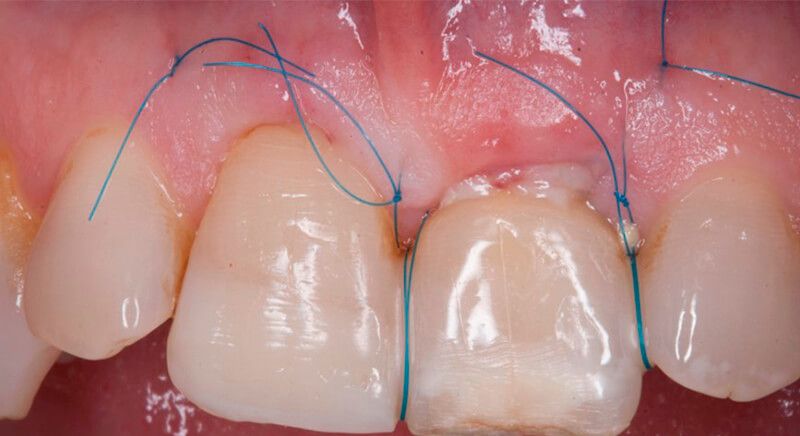
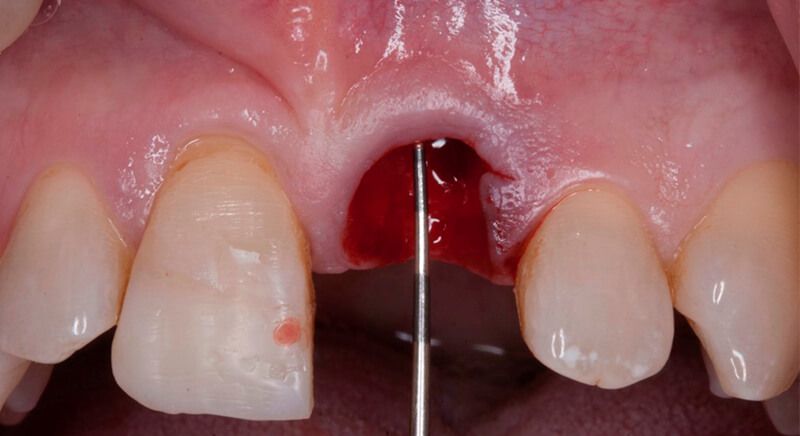
Once the hard and soft tissues had healed, 6 months after the surgery, a good volume remained in the vestibular area. It was then that we could consider an implant, using guided surgery to ensure it was placed in the correct three-dimensional position.
Tissue volume gained after socket preservation and mucogingival graft Tissue volume gained after socket preservation and mucogingival graft Tissue volume gained after socket preservation and mucogingival graft Tissue volume gained after socket preservation and mucogingival graft




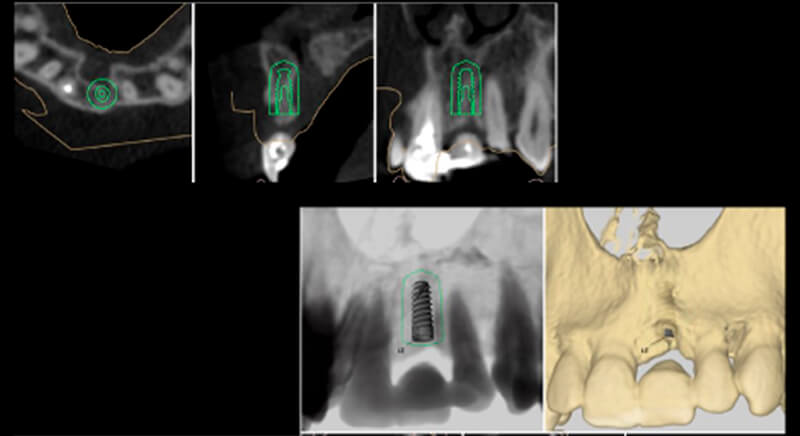
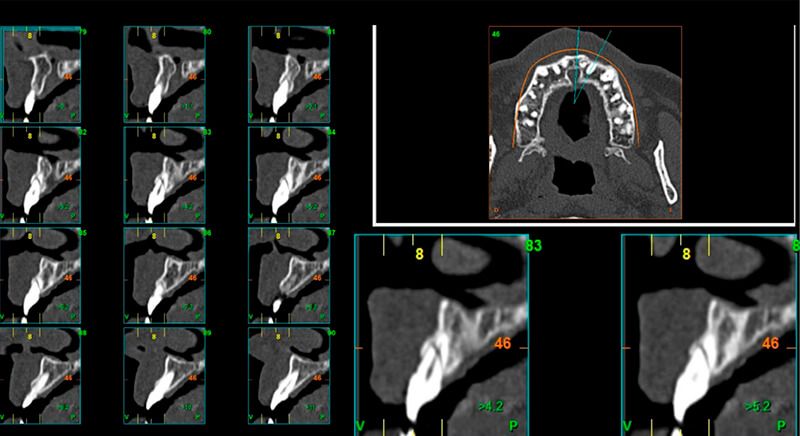
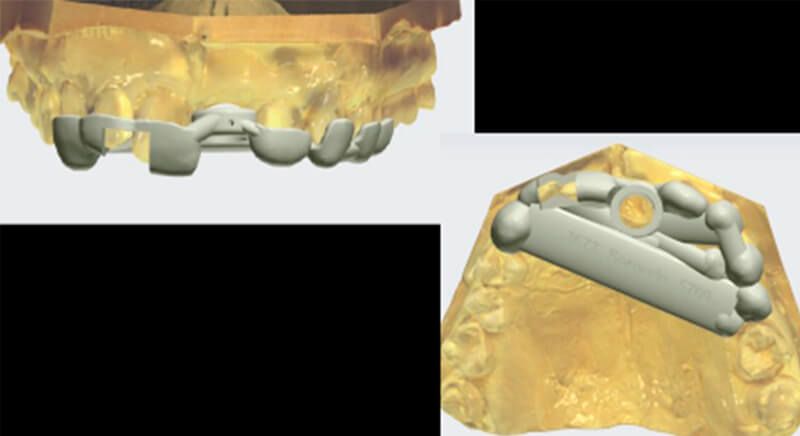
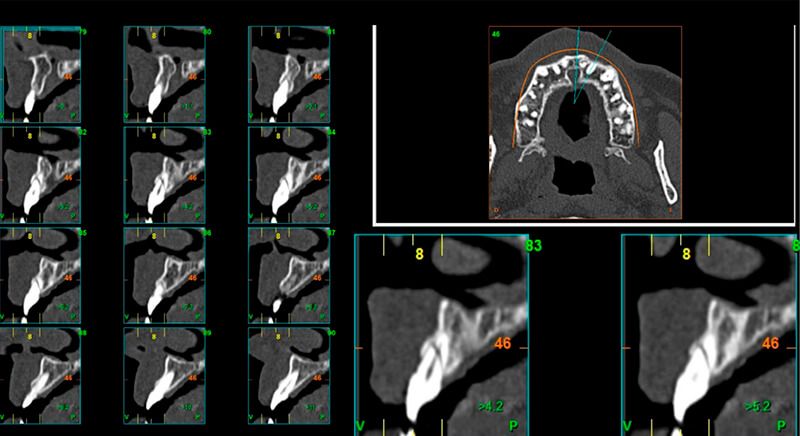
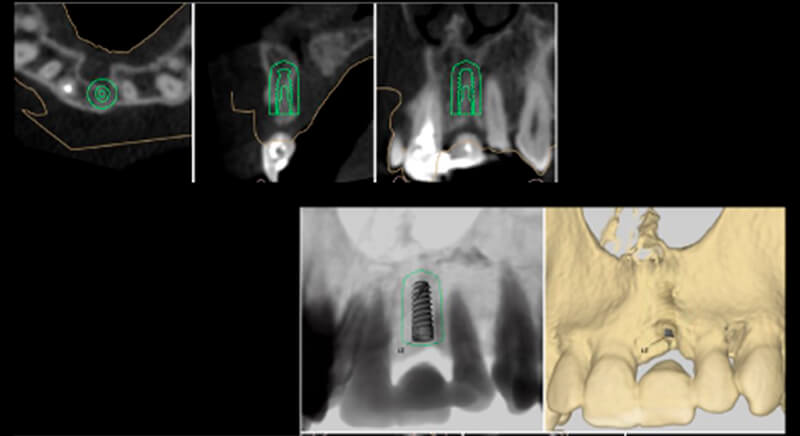
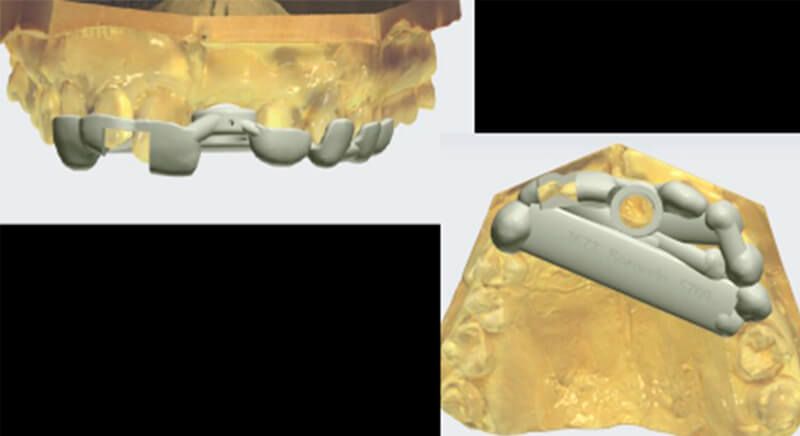
During the digital planning for the implant, with Implant Studio (3Shape) guided surgery software, significant bone defects due to the patient’s anatomy were discovered. Placing the implant in the correct position for the prosthesis presented bone dehiscence in the vestibular area, and another bone defect in the palatine area due to the patient’s large nasopalatine canal.
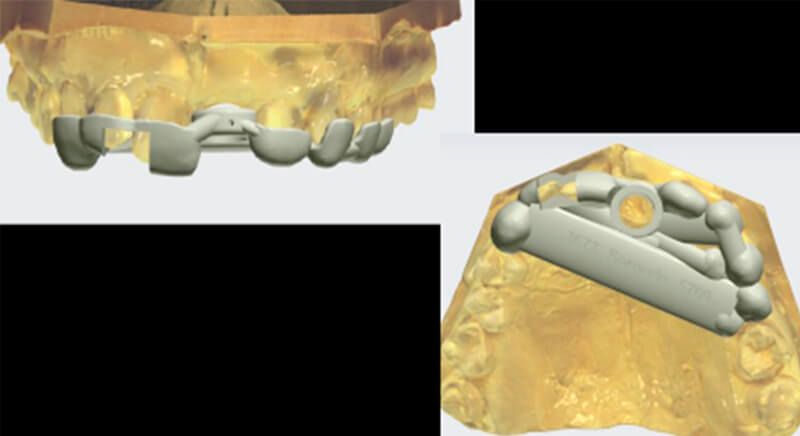
Planning the implant and details of the bone defects Designing the Avinent surgical guide
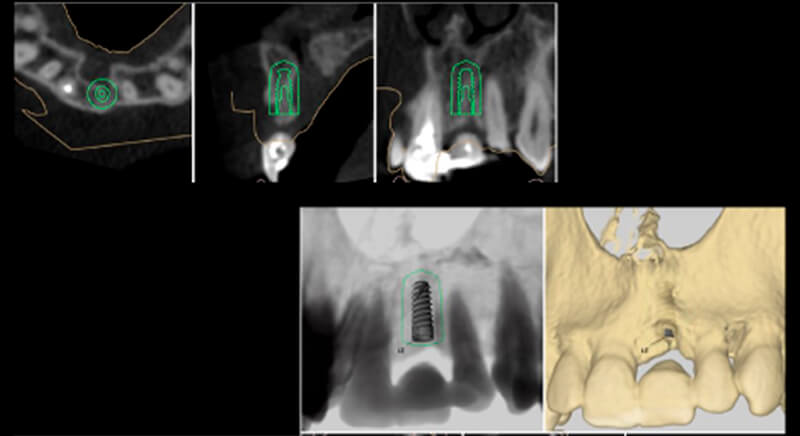
This information enabled us to rule out the option of surgery without a flap, as regeneration simultaneous to surgery would be needed, so the idea of using guided surgery was maintained.
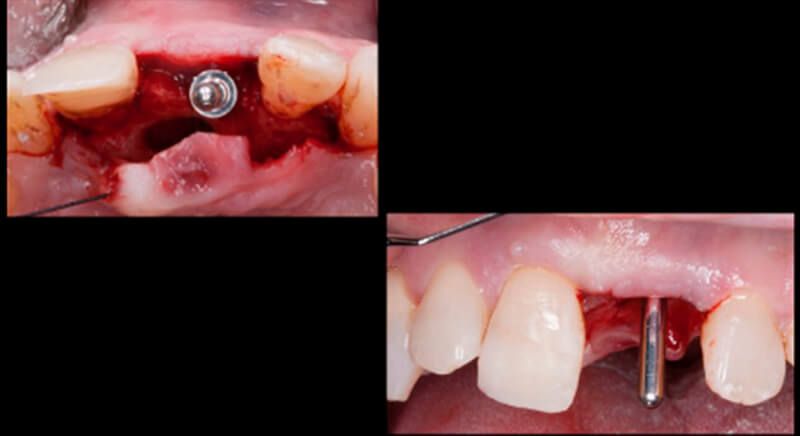
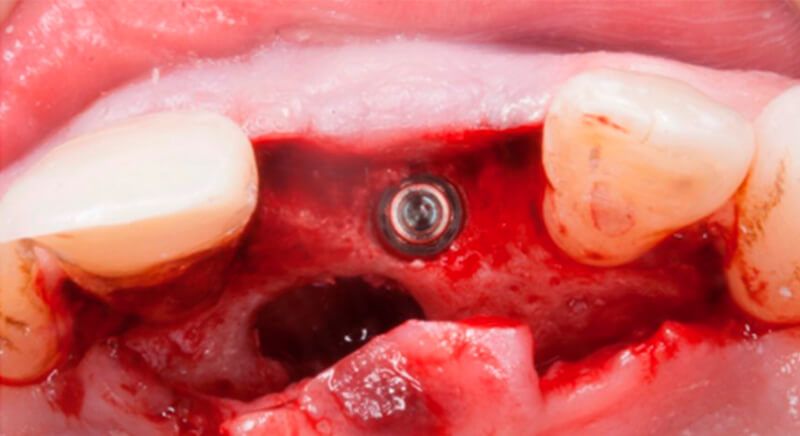
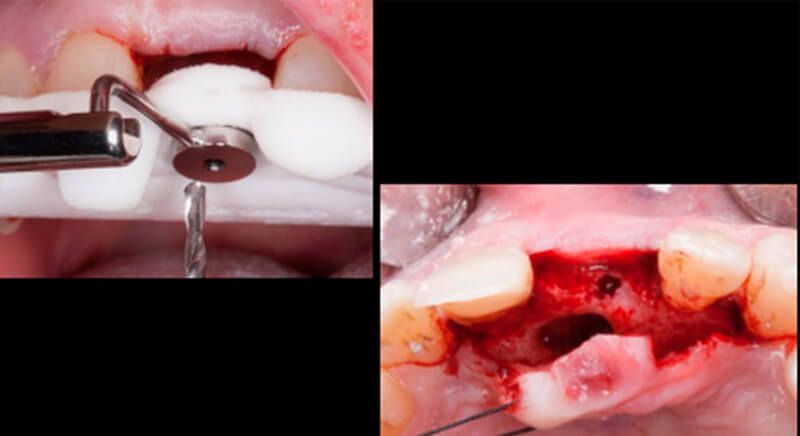
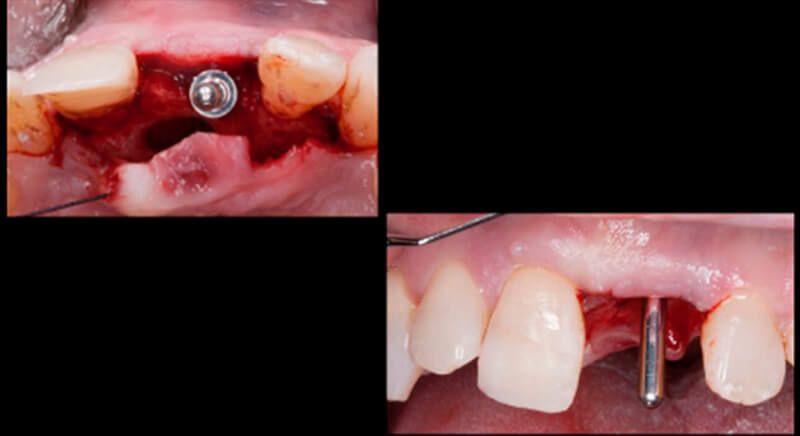
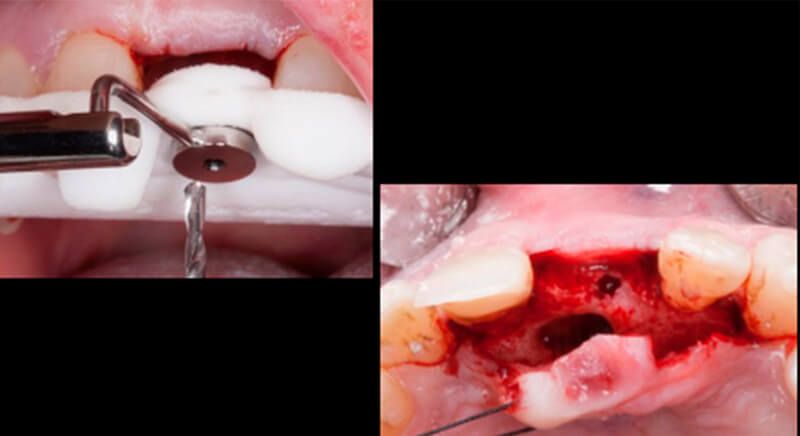
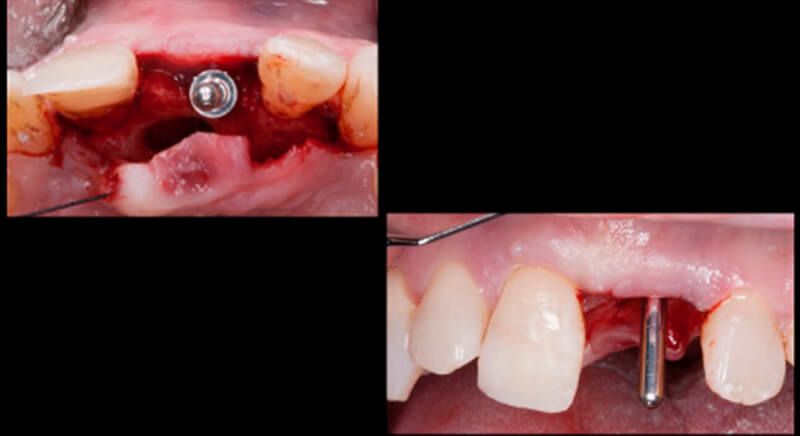
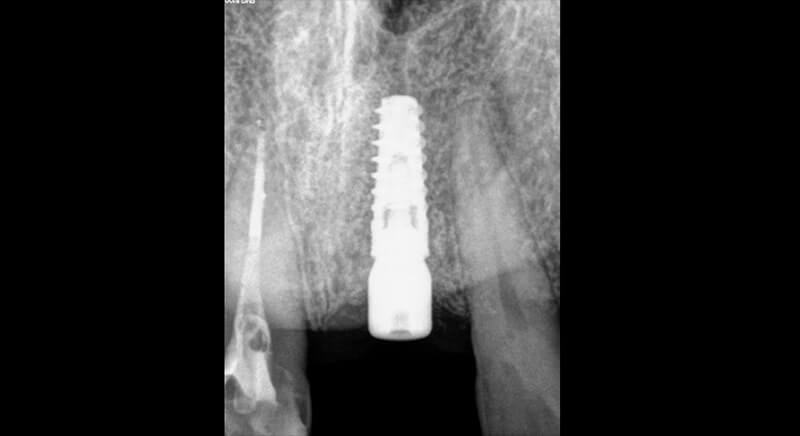
Clean nasopalatine canal Avinent surgical guide in position Drilling procedure for the guided surgery and placement of the implant Drilling procedure for the guided surgery and placement of the implant Three-dimensional position of the Biomimetic Ocean CC implant
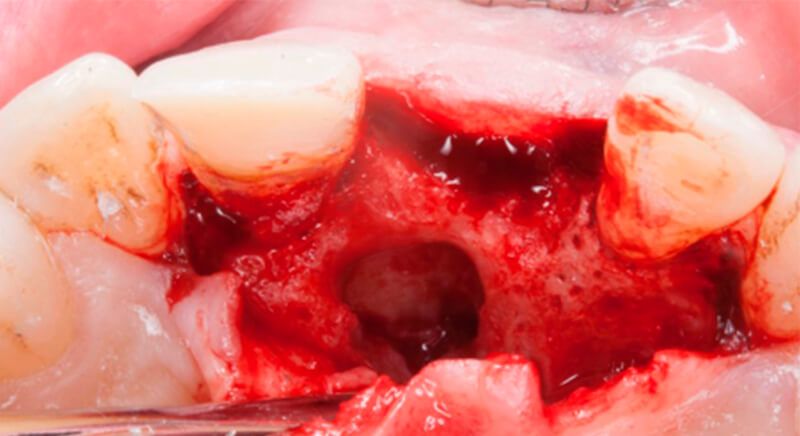

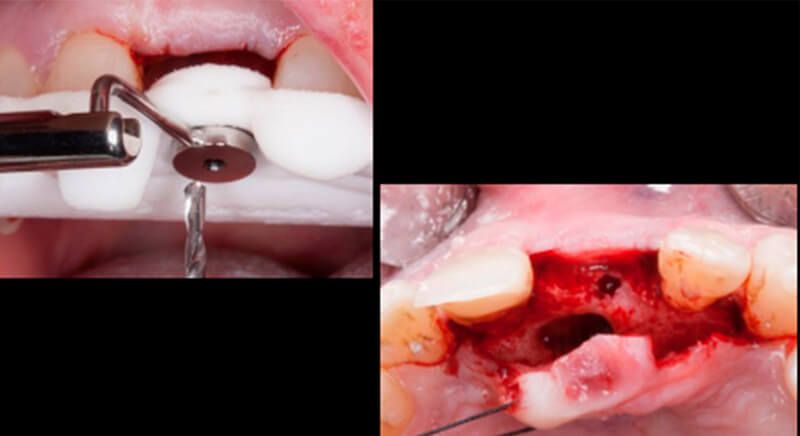
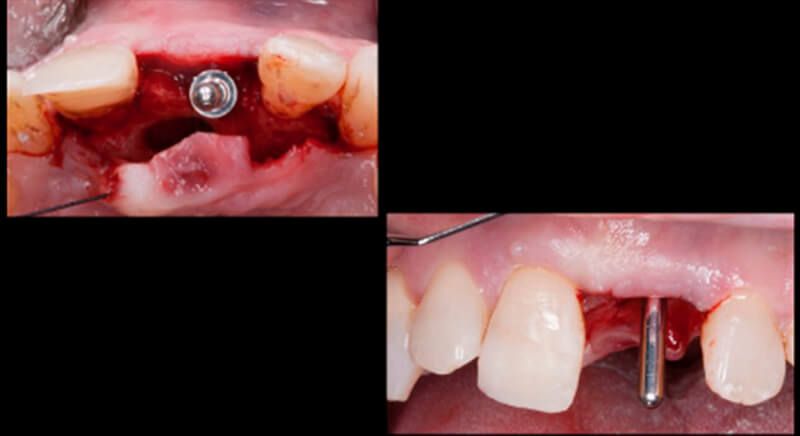
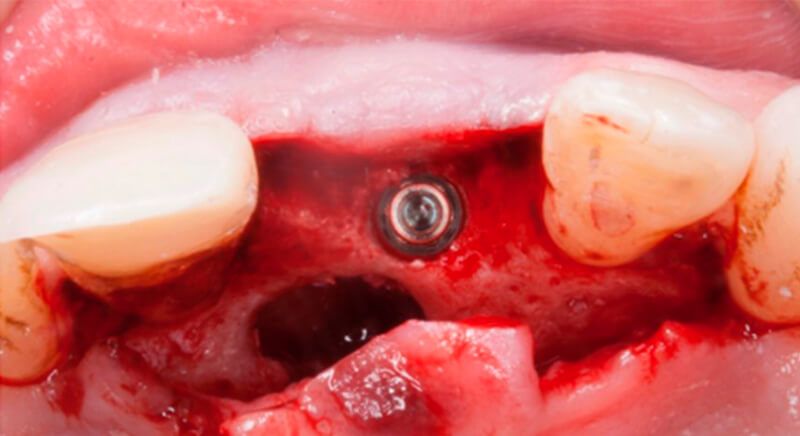
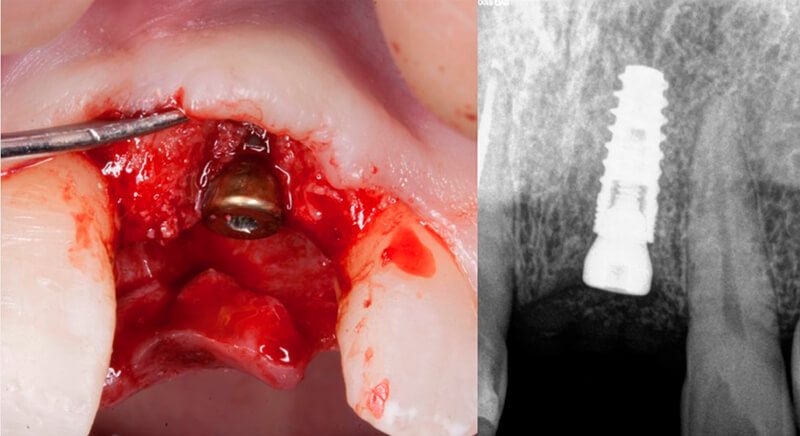
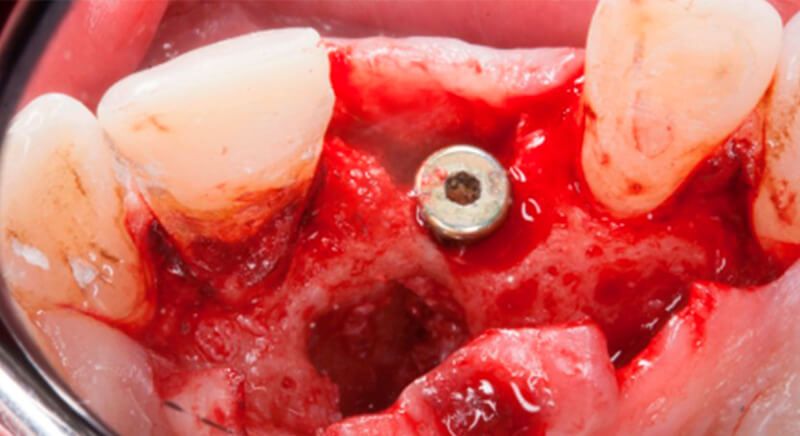
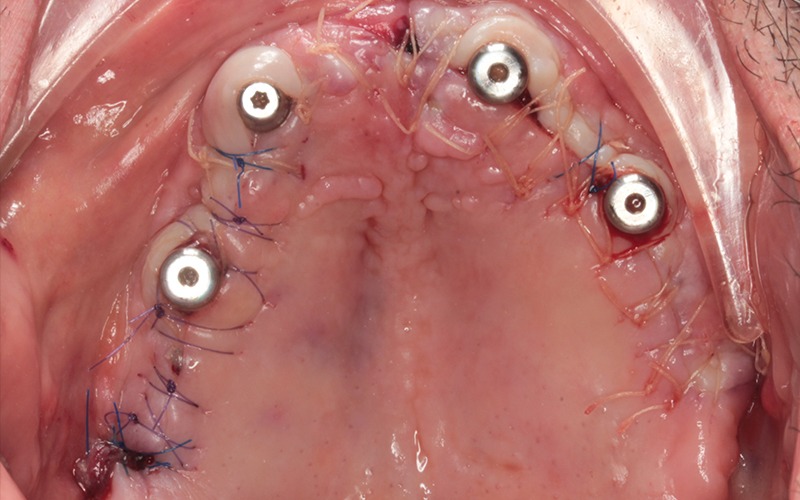
The guided surgery was performed by lifting a full thickness mucoperiosteal flap. A Biomimetic Ocean CC implant, diameter 3.5mm and length 10mm, was inserted using the surgical guide in the ideal three-dimensional position and the defects were regenerated with xenograft and reabsorbable membrane, the nasopalatine duct on the palatine side and the area of dehiscence on the vestibular.
During the same surgical intervention, a short 3mm Avinent healing abutment was positioned and fully covered by the flap. Primary closure was completed and we waited 6 months for the bone graft to mature.
Sequence of the bone defect regeneration using xenograft and reabsorbable membrane Sequence of the bone defect regeneration using xenograft and reabsorbable membrane Sequence of the bone defect regeneration using xenograft and reabsorbable membrane


Closure of the tissues during the surgery Closure of the tissues during the surgery Healing of the soft tissues after 15 days, after suture removal, and the same Maryland type provisional cemented to the adjacent teeth Healing of the soft tissues after 15 days, after suture removal, and the same Maryland type provisional cemented to the adjacent teeth


Images at 6 months after implant placement, showing correct healing of the soft tissues and satisfactory vestibular volume, in the area of both tooth 1.1 and the implant 2.1. Images at 6 months after implant placement, showing correct healing of the soft tissues and satisfactory vestibular volume, in the area of both tooth 1.1 and the implant 2.1. Images at 6 months after implant placement, showing correct healing of the soft tissues and satisfactory vestibular volume, in the area of both tooth 1.1 and the implant 2.1.



After 6 months of healing, a minimum crestal incision was made to change the 3mm abutment underneath for a 5mm abutment that would be exposed to the oral medium.
Finally, a definitive metal ceramic crown was designed and manufactured for 2.1 and a veneer for 1.1.
Preparation of the veneer for 1.1 Placing the crown for 2.1 Placing the crown for 2.1 Definitive prosthesis in the mouth Before and after the treatment





Conclusions
Tooth loss can cause dimensional changes to both hard and soft tissues that affect the patient’s final appearance, above all with treatments in the anterior sector.
If the treatment also includes dental implants, a correct diagnosis of the defect, good planning of the three-dimensional position of the implants, selection of the surgical technique and treatment of the soft tissues during the provisional restoration are important for predictable aesthetic results.
This clinical case shows the anticipation of the changes in volume that are going to occur after the dental extraction in terms of both bone and soft tissues.
Moreover, guided surgery makes it possible to place the implant in the correct three-dimensional position, despite unfavourable bone anatomy.




Initial image of the case X-ray images of the initial status IX-ray images of the initial status Details of the reconstructed tooth Details of the reconstructed tooth Sequence of images during the extraction of tooth 2.1. Sequence of images during the extraction of tooth 2.1. Sequence of images during the extraction of tooth 2.1. Sequence of images during the extraction of tooth 2.1. Placing the xenograft Incision in the donor area of the palate Incision in the donor area of the palate De-epithelialized lamina propria graft
Sequence of the socket preservation technique and placement of the connective tissue graft
Sequence of the socket preservation technique and placement of the connective tissue graft
Sequence of the socket preservation technique and placement of the connective tissue graft
Sequence of the socket preservation technique and placement of the connective tissue graft
Sequence of the socket preservation technique and placement of the connective tissue graft
Placing the aesthetic Maryland-type immediate-load provisional and suturing the graft
Placing the aesthetic Maryland-type immediate-load provisional and suturing the graftX-ray of the regeneration and the provisional without load Healing of the donor and receiving areas 7 days after the mucogingival surgery State of the tissues after 15 days Final removal of the sutures
Tissue volume gained after socket preservation and mucogingival graft
Tissue volume gained after socket preservation and mucogingival graft
Tissue volume gained after socket preservation and mucogingival graftTissue volume gained after socket preservation and mucogingival graft Planning the implant and details of the bone defects Designing the Avinent surgical guide Clean nasopalatine canal Avinent surgical guide in position Drilling procedure for the guided surgery and placement of the implant Three-dimensional position of the Biomimetic Ocean CC implant Three-dimensional position of the Biomimetic Ocean CC implant Placing the healing abutment Sequence of the bone defect regeneration using xenograft and reabsorbable membrane Sequence of the bone defect regeneration using xenograft and reabsorbable membrane Sequence of the bone defect regeneration using xenograft and reabsorbable membrane Closure of the tissues during the surgery Closure of the tissues during the surgery
Closure of the tissues during the surgeryHealing of the soft tissues after 15 days, after suture removal, and the same Maryland type provisional cemented to the adjacent teeth Images at 6 months after implant placement, showing correct healing of the soft tissues and satisfactory vestibular volume, in the area of both tooth 1.1 and the implant 2.1. Images at 6 months after implant placement, showing correct healing of the soft tissues and satisfactory vestibular volume, in the area of both tooth 1.1 and the implant 2.1. Images at 6 months after implant placement, showing correct healing of the soft tissues and satisfactory vestibular volume, in the area of both tooth 1.1 and the implant 2.1. Fit of the healing abutment Preparation of the veneer for 1.1 Placing the crown for 2.1 Placing the crown for 2.1 Definitive prosthesis in the mouth Before and after the treatment Prosthetic restoration 1 year after treatment Prosthetic restoration 1 year after treatment X-ray of the implant after 2 years Stability of the hard and soft tissues after two years